
A 63-year-old man, with a long history of commercial poultry processing, was admitted to the intensive care unit with fever and cough for 6 days after breeding and selling pigeons. He had a previous history of tuberculosis, which was cured by anti-tuberculosis medication. In the last month, there was a gradual onset of discomfort with dry eyes and dry mouth. On examination, he had low breath sounds in the left lung with significant wet rales. Laboratory tests revealed that his white blood cell count, erythrocyte sedimentation rate, C-reactive protein, and calcitonin were significantly elevated. Blood gas analysis revealed refractory type I respiratory failure with poor mechanical ventilation. Salivary flow rate and Schirmer’s test confirmed the presence of primary Sjögren’s syndrome. A chest computed tomography scan and X-ray demonstrated infiltration and consolidation of the left lower lung (Figures 1 A, B). Metagenomic next-generation sequencing analysis of bronchoalveolar lavage fluid revealed a specific sequence number of 531 for Chlamydia psittaci (SRX9416611), demonstrating the presence of Chlamydia psittaci infection in the patient [1, 2]. The final diagnosis of primary Sjögren’s syndrome combined with psittacosis was made. Treatment with doxycycline 100 mg twice daily for psittacosis, prednisolone 30 mg once daily in combination with hydroxychloroquine 200 mg twice daily for primary Sjögren’s syndrome was initiated, leading to a remarkable improvement in laboratory findings and symptoms. The imaging results revealed gradual absorption of the left lung infiltration 1 week later (Figures 1 C, D).
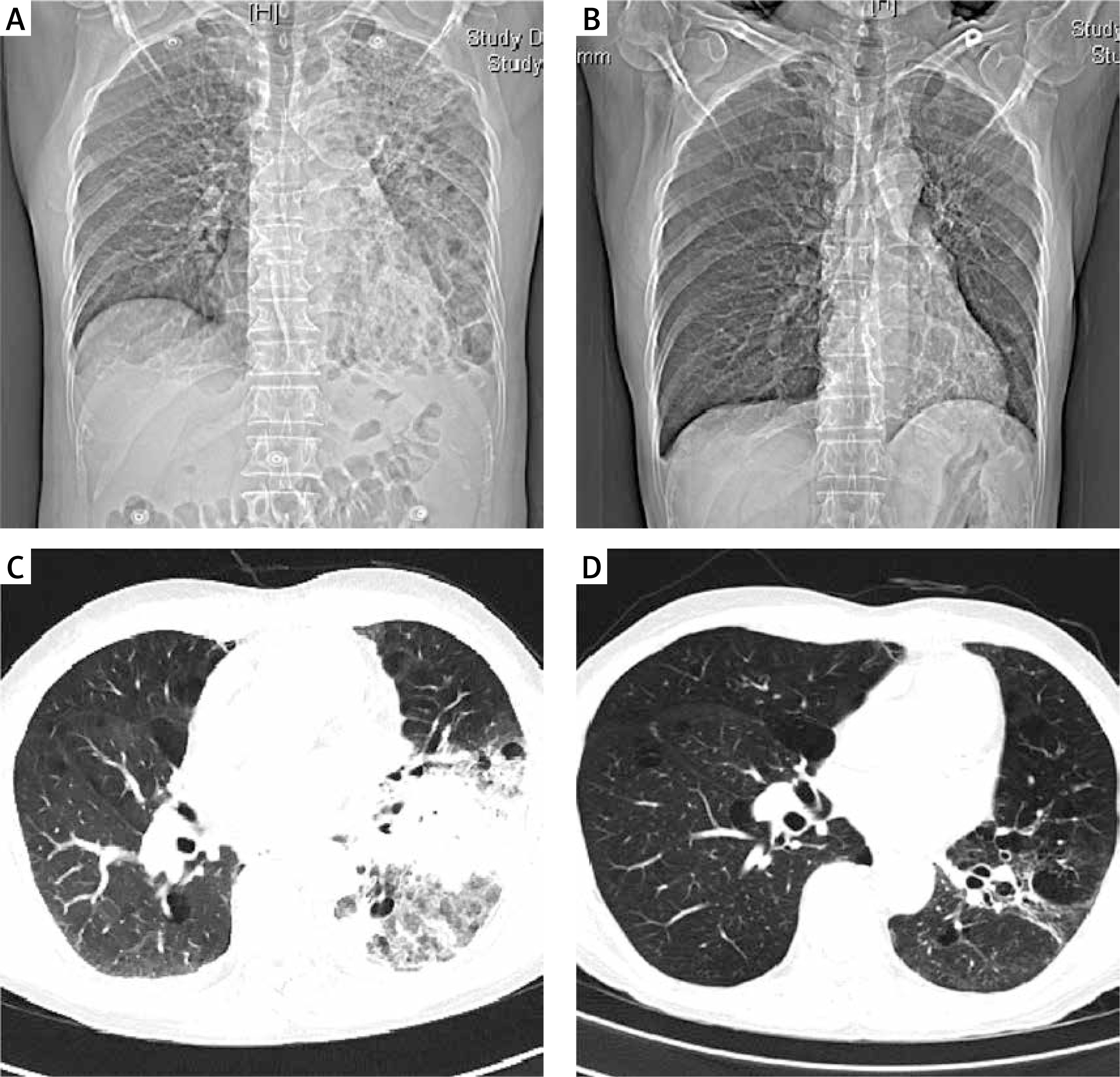
Figure 1
A, B – Computed tomography and radiographs showing massive infiltration and consolidation of the left lower lung. C, D – Computed tomography and radiographs showing gradual absorption of the infiltrate in the left lower lung after treatment
Psittacosis is a zoonotic disease caused by Chlamydia psittaci [3, 4]. Patients infected with Chlamydia psittaci have infiltration and exudation of inflammatory cells in the alveoli, resulting in significant thickening of the alveolar wall and interstitial lung mass, edema, and necrosis [5]. In addition, the primary Sjögren’s syndrome can also lead to interstitial pulmonary fibrosis [6]. The respiratory symptoms in this patient resulted from the absence of mucus in the airways and the formation of inflammatory infiltrates within the lungs in the late stage of the disease, resulting in extremely poor pulmonary ventilation and gas exchange as well as refractory type I respiratory failure. To our knowledge, there are no reports of Chlamydia psittaci infection in patients with primary Sjögren’s syndrome. Clinicians should pay close attention to the pulmonary status of patients with autoimmune diseases and be especially alert for infections with atypical pathogenic bacteria [7].