According to the European Observatory of Health Systems and Policy, international migration of health workers should become a key component of the health policy at the present time [1, 2]. This statement, on the one hand, is based on United Nations data relating to aging of the global population [3], which means that more and more people will demand medical care, and on the other hand, it is based on WHO data relating to the chronic shortage of health workers in many countries around the world [4]. In the next 25 years, the proportion of people aged 60 or over of the world population will increase from nearly 12% (2013) to approximately 21% (2050) [3]. Satisfying the demand for health services requires, first of all, ensuring a sufficient number of health workers [4]. But here is the problem: the generation gap of the health workforce. In Poland, human resources (doctors and nurses) in health care are critically low (the ratio of health workers to population) compared to other EU countries [5, 6]. According to Eurostat estimates, the percentage of people aged 65+ in the Polish population will reach 34.5% in 2060 (13.5% in 2010). It means that Poland is currently one of the youngest EU countries, but in the long-term perspective, Poland will become one of the oldest populations of the EU [7]. Imposing the current level of human resources (nurses and doctors) in the Polish healthcare system on the upcoming demographic changes, it seems that the ability of the Polish healthcare system to meet the future needs of the aging population will undoubtedly be a huge challenge (in terms of providing sufficient human resources) for health policy makers in Poland [5–7]. Due to the chronic shortage of health workers [4–6], migration of nurses and doctors may be crucial in the near future. But this migration from Poland is not monitored in a reliable way, and for this reason, official data on migration of nurses and doctors, at approximately 7% of those engaged in the occupation in the years 2004–2014 [8, 9], should be treated only as an estimate of the willingness to work abroad and not the real migration scale of Polish health workers. Our study aimed to gain knowledge not only about the scale of migration among Warsaw doctors and nurses, but also the motives and barriers of migration, directions and temporary nature of migration. Our study aimed to identify the factors that influence nurses’ and doctors’ decisions to migrate from Poland.
Paper-based, self-administered anonymous questionnaires were personally distributed to physicians and nurses in Warsaw’s public medical entity between the 14th of October 2013 and the 30th of March 2014. The research method was based on the availability of respondents. Questionnaires were distributed in an amount equal to the number of employed doctors and nurses. Migration intentions were assessed by asking the question, “Do you intend to go to another country to work there in your profession?”. Answer choices were (1) yes, (2) no, (3) yes, but not as a nurse. This form of question follows from the phenomenon of Polish nurses taking up work abroad as nursing assistants (before qualification), while such a phenomenon has no equivalent in the case of doctors. Other questions related to: (1) destination country of migration, (2) the temporary nature of migration and the characteristics of socio-demographic factors, such as, (3) place of work – qualitative dichotomous variable, (4) education – ordinal variable, (5) age – ordinal variable, (6) net income per family member – ordinal variable, (7) working time in hours per month – quantitative variable, (8) the period of employment in the profession at all and (9) the current place of work – both quantitative variables, (10) participation in meetings of recruitment companies – qualitative dichotomous variable, (11) the presence of family/friends abroad – ordinal variable, and (12) experience of working abroad – qualitative dichotomous variable. Logistic regression was undertaken to determine whether socio-demographic factors are associated with migration intentions. The analysis aimed to design multidimensional models based on logistic regression for a binary dependent variable – the decision to migrate. Designed models included V-fold cross validation. Separate multivariate models were constructed separately for doctors and nurses. Statistica v.12 StatSoft was used for data analysis. The study was approved by the director of the relevant unit of the capital city of Warsaw – Office of Health Policy.
The survey was distributed to 2163 medical professionals (physicians and nurses) employed in Warsaw public medical entities (6 hospitals, 39 outpatients clinic and 1 long-term care home). The response rate was 50% (n = 1071). The response rate varied between medical entity, ranging from 30% to 80%. The study was conducted in 8 of the 18 districts of the capital city of Warsaw: (1) Bielany, (2) Białołęka, (3) Żoliborz, (4) Wola, (5) Ochota, (6) Mokotów, (7) Praga Południe, (8) Śródmieście.
Table I lists the key characteristics of all respondents (migrants and non-migrants). Based on these data, logistic regression was performed to assess factors contributing to the decision to migrate.
Table I
Demographic characteristics of survey respondents (physicians n = 374 ; nurses n = 697)
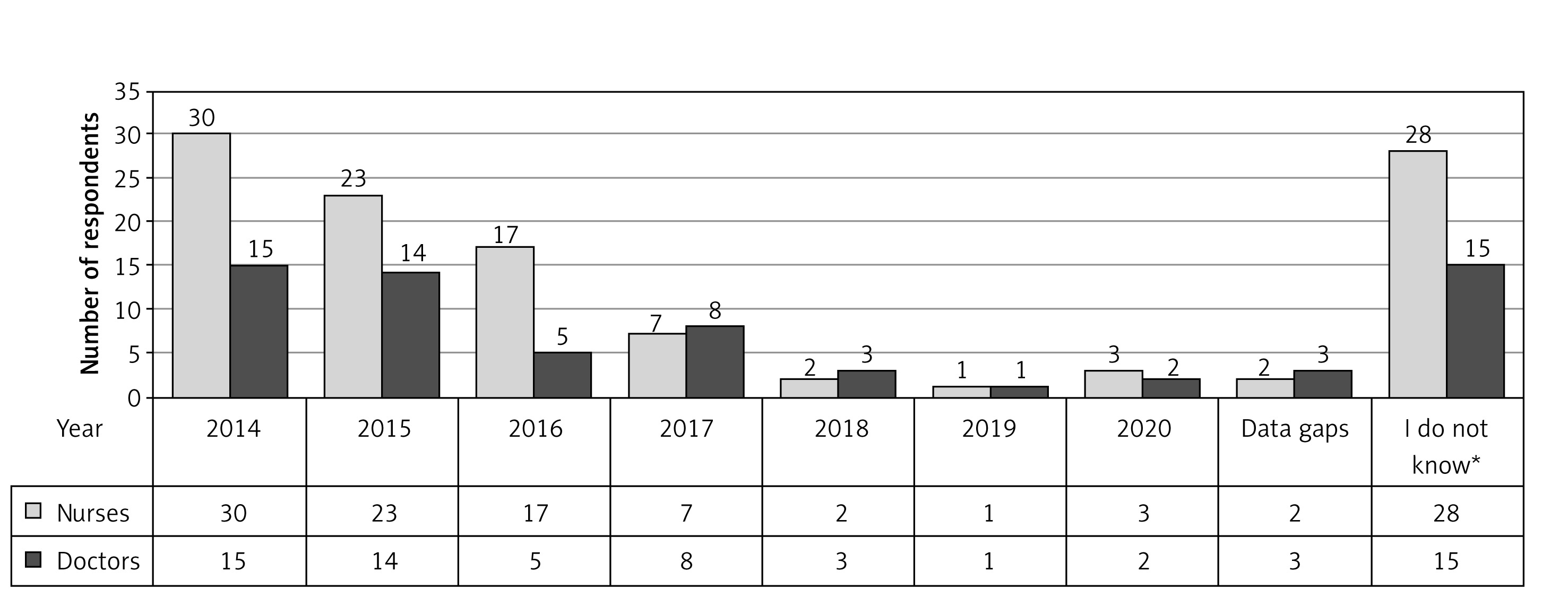
In the present study, 16% of physician (n = 60/374) and 15% of nurses (102/697) declared their intention to leave Poland in the years 2014–2020 to take up work abroad. Most of the respondents intend to leave Poland in the years 2014–2017. One quarter of migrating nurses (n = 28/102) and one quarter of migrating physicians (n = 15/60) do not know when they will move abroad, but certainly will do so by 2020 (detailed in Figure 1).
Figure 1
Question: Please provide the year in which you will leave Poland. Attention! Multiple answers are possible. (Semi-open question, does not add up to 100%)
*I do not know, but I am going to leave Poland by 2020.
Fifty-five percent of migrating nurses (n = 56/102) and 47% of migrating doctors (n = 28/60) do not know whether their leave Poland will be of a single or a multiple nature.
Fifteen percent of migrating nurses (n = 15/102) and 12% migrating doctors (n = 7/60) chose the answer that their migration will be of a single nature; i.e. firstly, after some time, they will return to Poland (nurses – 40%, n = 6/15, doctors – 13%, n = 1/7); secondly, will they leave Poland permanently (nurses – 60%, n = 9/15, doctors – 86%, n = 6/7).
Thirty percent of migrating nurses (n = 30/102) and 40% of migrating doctors (n = 24/60) chose the answer that their migration will be of a multiple nature; i.e. firstly they will move from Poland to another country many times and each time it will be the same country (nurses – 67%, n = 20/30, doctors – 63%, n = 15/24); secondly, they will move from Poland to another country many times and each time it will be a different country (nurses – 30%, n = 9/30, doctors – 33%, n = 8/24). Missing data for this question amounted to 3% (n = 1/30) for nurses and 4% (n = 1/24) for physicians.
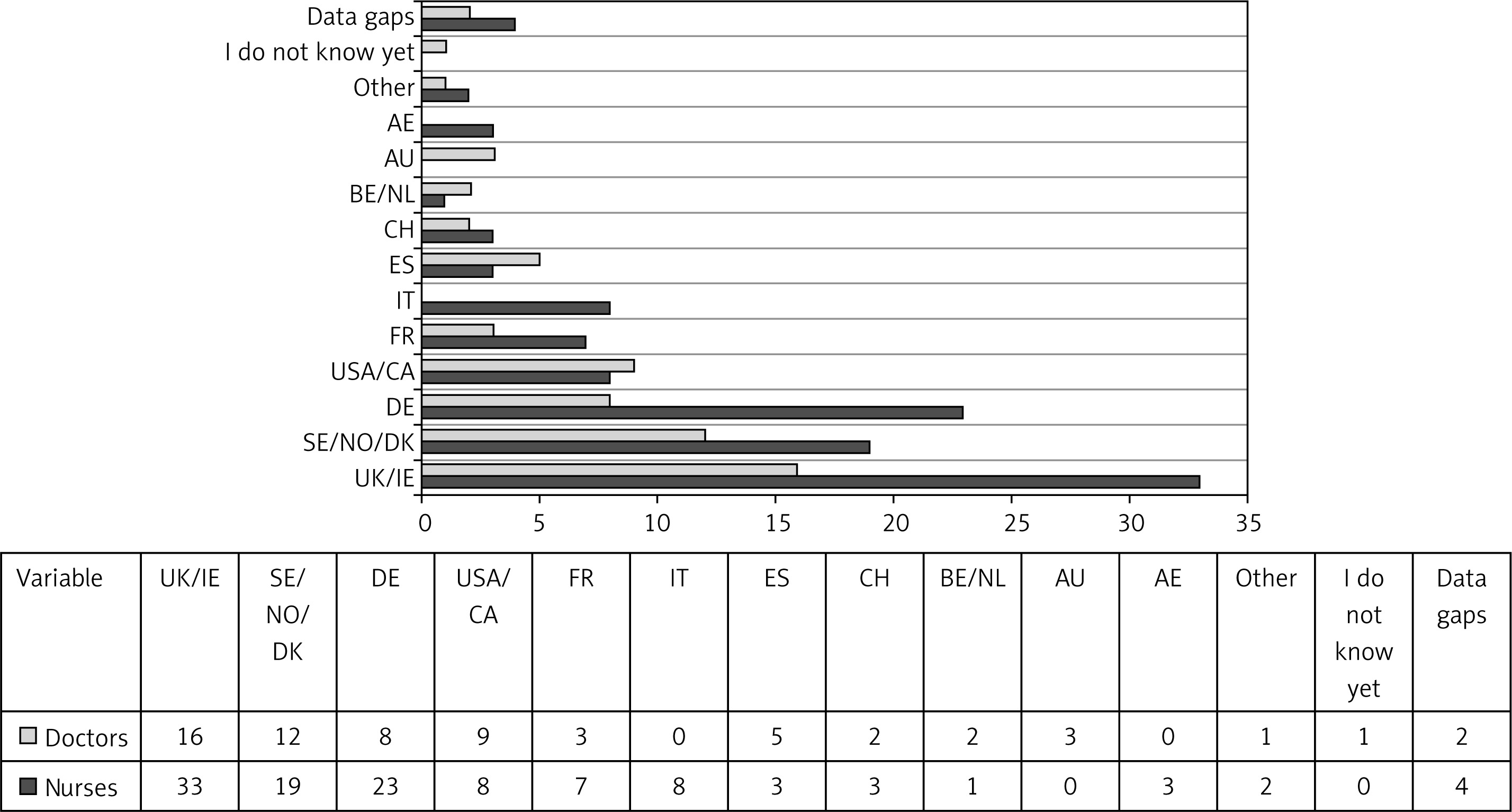
Nurses and physicians indicated mainly the United Kingdom (UK) and Ireland (IE), about one-quarter of physicians (27%, n = 16/60) and one-third of nurses (32%, n = 33/102); the second most common direction of migration was the Scandinavian countries, i.e. Sweden (SE), Norway (NO) and Denmark (DK), about one-fifth of physicians (20%, n = 12/60) and about one-fifth of nurses (19%, n = 19/102); likewise, the second most common direction of migration was Germany (DE), but Germany more often was indicated by nurses (23%, n = 23/102) than physicians (13%, n = 8/60) (detailed in Figure 2).
Figure 2
Question: Which country will be your destination country of migration in the near future? Multiple answers are possible (open question; does not add up to 100%; n = 102 nurses, doctors, n = 60)
*Other (New Zealand, Finland, Austria)
The question concerning motives of the declared migration was an open-ended question. Respondents’ answers were assessed in the course of the qualitative evaluation by one of the researchers. The qualitative analysis used open/explorative coding – after the qualitative analysis of the respondents’ answers was carried out, a categorisation key was constructed (Table II). The questions were addressed at respondents who declared that they would leave Poland (nurses, n = 102; physicians, n = 60).
Table II
Motives of declared migration classified according to the category key developed by the authors of the work in the course of qualitative analysis of the responses
The question concerning migration barriers among respondents who declared that they would stay in Poland (non-migrants) was an open-ended question. Respondents’ answers were assessed in the course of the qualitative evaluation by one of the researchers. The qualitative analysis used open/explorative coding – after the qualitative analysis of the respondents’ answers was carried out, a categorisation key was constructed (Table III). The questions were addressed to respondents who declared that they would stay in Poland (nurses, n = 595; physicians, n = 314).
Table III
Migration barriers classified according to the category key developed by the authors of the work in the course of qualitative analysis of the responses
The study was conducted with the objective of identifying predictors for leaving Poland to work abroad as a nurse or a medical doctor. Nine variables were analysed by logistic regression – (1) education degree, (2) age, (3) net income in household per family member, (4) participation in meetings of recruitment companies, (5) experience of working abroad, (6) family or friends abroad, (7) average monthly hours worked, (8) work experience (in years), (9) years in current place of work. Only three variables were found to be statistically significant, i.e. participation in meetings of recruitment companies, experience of working abroad, and work experience.
The multivariate logistic regression model including all of the demographic factors listed above revealed that:
doctors who reported participation in meetings of recruitment companies were more likely to be considering leaving Poland (odds ratio = 3.5, 95% confidence interval (CI): 1.462–8.483, p = 0.005),
doctors who reported experience of working abroad were more likely to be considering leaving Poland (odds ratio = 5.5, 95% CI: 2.141–13.953, p < 0.001),
In the sample of doctors, variable work experience (in years) decreases the likelihood of the decision to leave Poland. An increase of one unit of variable work experience (in years) decreases by around 11% the likelihood of considering leaving Poland.
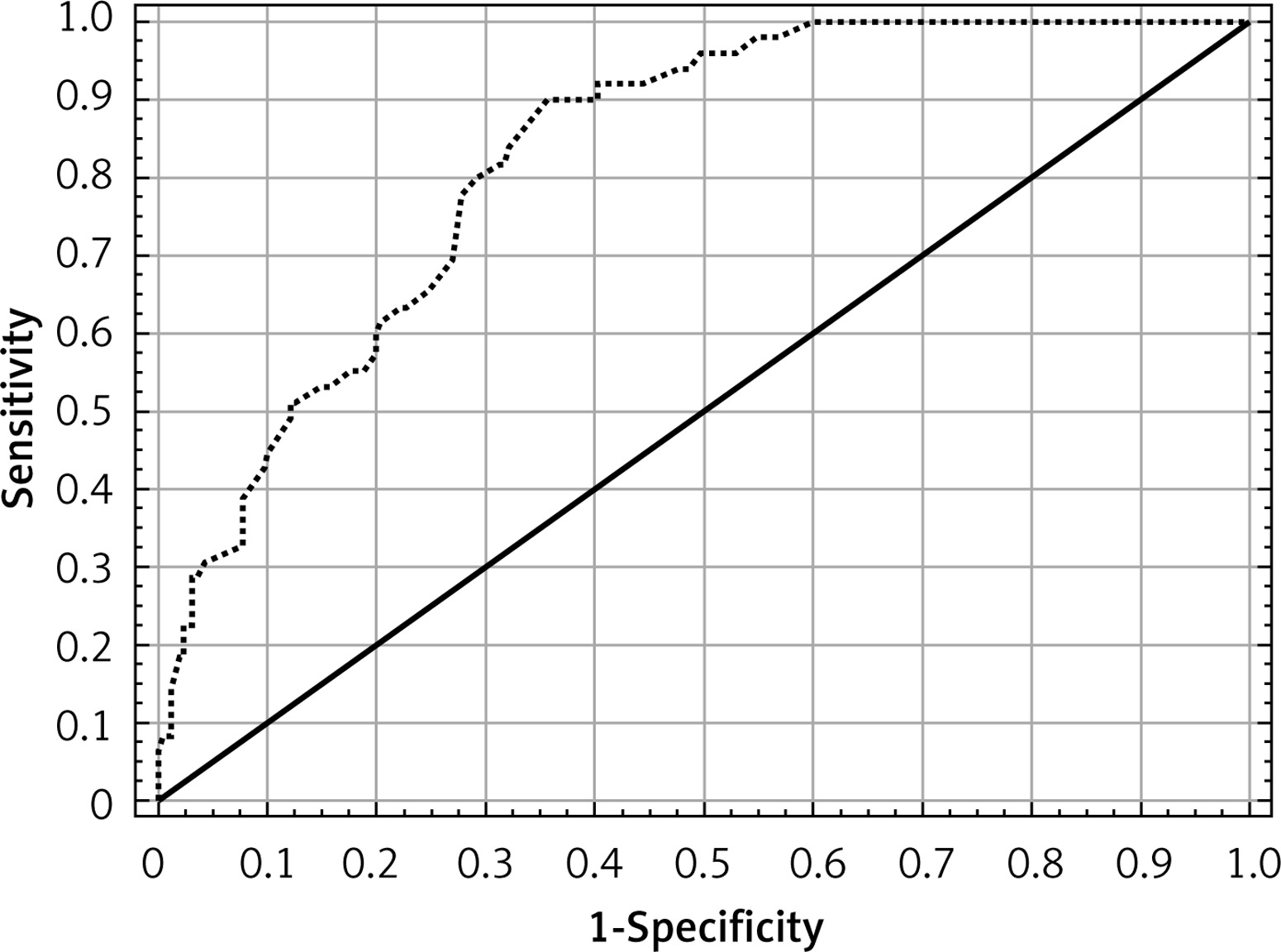
For multivariate analysis, the Hosmer and Lemeshow χ2 test for goodness of fit was applied for testing the model fit. It was found to be significant (p-value= 0.25, Hosmer-Lemeshow χ2 statistic = 8.95) and area under the curve (AUC = 0.82) leads to the conclusion that there are no grounds to conclude that the model is ill-fitting and is also confirmed in the following interpretation in the form of the ROC curve (Figure 3).
The multivariate logistic regression model including all of the demographic factors listed above revealed that:
nurses who reported participation in meetings of recruitment companies were more likely to be considering leaving Poland (odds ratio = 4.129, 95% CI: 2.088–8.167, p < 0.001),
doctors who reported experience of working abroad were more likely to be considering leaving Poland (odds ratio = 3.545, 95% CI: 1.636–7.681, p = 0.001),
In the sample of doctors, variable work experience (in years) decreases the likelihood of the decision to leave Poland. An increase of one unit variable work experience (in years) decreases by around 9% the likelihood of considering leaving Poland.
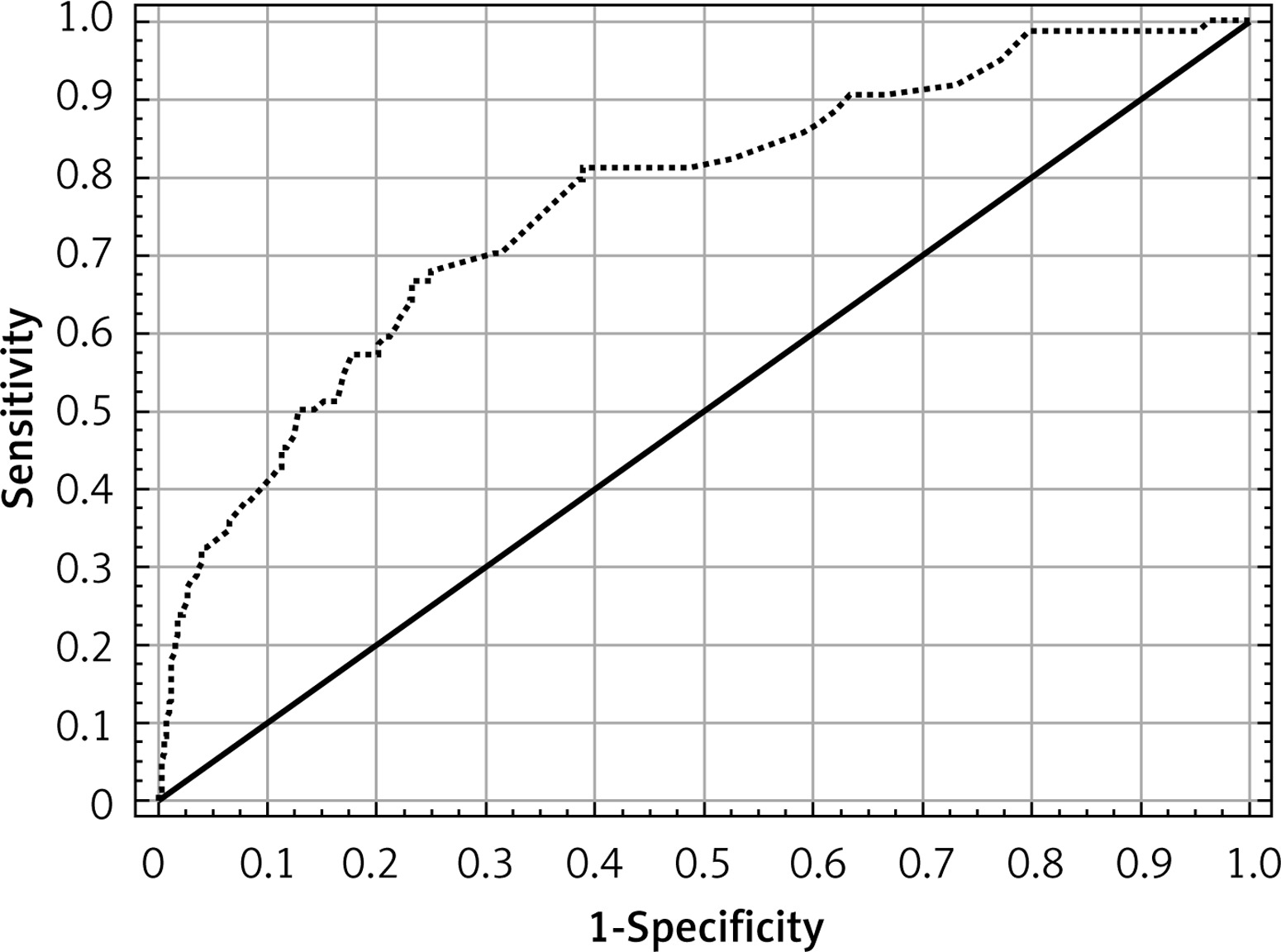
For multivariate analysis, the Hosmer and Lemeshow chi-square test for goodness of fit was applied for testing the model fit. It was found to be significant (p = 0.18, Hosmer-Lemeshow χ2 = 11.35) and area under the curve (AUC = 0.77) leads to the conclusion that there are no grounds to conclude that the model is ill-fitting and is also confirmed in the following interpretation in the form of the ROC curve (Figure 4).
This survey study of Warsaw’s medicine doctors’ and nurses’ migration is a first look into the migration of health workers on a local (city) or on any other level in Poland. The authors of this study did not find any other original study in this matter (Polish context) in worldwide scientific literature (PubMed). So, for this reason, in our study, no comparisons were made in the context of migration of nurses and doctors from other Polish regions, which would be the most appropriate comparisons, assuming a relatively homogeneous nature of the migration of Polish health workers.
In the present study, the scale of migration of doctors and nurses in the Warsaw sample may seem small (around 15%), but given the demographic changes, resulting in overall aging of Polish citizens [10], not only the health care workers [11], perhaps this 15% is more than it seems. The aging of society has a twofold effect on the health safety of the country. On the one hand, the population is aging, so this increases the demand for health care services, and on the other hand, the medical staff is aging, and therefore it declines in the labour market, so the supply of medical services decreases. So, considering the above context, the migration of 15% may be significant at a local level. Migration of health workers can be damaging not only for big cities like Warsaw, but also for small and medium-sized cities where access to specialist services can be difficult. From a logical point of view, when migration occurs from large cities to other countries, at the same time, it should be seen as the smaller towns following the migration of large urban centres [12].
It is worth mentioning that the responses are only declarations. So, how to check whether the declaration is going to happen? It is not possible, but if we analyse the responses concerning the year of leaving Poland, then we can presume that only one quarter of respondents do not have more specific plans for the migration, which suggests that these people are less likely to migrate. If this assumption proves true, then the scale of the potential migration of Warsaw’s nurses and doctors will drop from 15% to 12%.
Most of the migrating respondents, after their period of stay abroad, do not know what they will do – nearly half of them. Almost one third of migrating respondents stated that they will migrate many times (Poland – destination country/countries). One in ten migrating respondents stated that they will stay abroad permanently. This brief summary of our results showed that a significant proportion of the respondents may fear that they will encounter obstacles. We can only speculate on the reasons – mental, cultural or linguistic?
In this study, the direction of nurses’ and doctors’ migration is primarily the United Kingdom and Ireland, then in equal numbers Scandinavian countries and Germany, which is a traditional country for the emigration of Poles [10]. Germany is gradually losing its importance in the context of Poles’ migration, since Poland acceded to the European Union [10]. This can also be observed in our study, where Germany was indicated by Warsaw’s nurses and doctors in the same place as Scandinavian countries. Migration to Germany has decreased mainly due to the opening of the labour market by the United Kingdom and Ireland in 2004 [10]. The high rank of the Scandinavian countries in our study is nothing new, if we keep in mind the data from the Central Statistical Office (Poland) [11]. Migration directions of Warsaw’s sample of medical doctors and nurses were not different from each other. Both professional groups chose the same countries. This refers to countries with higher GDP per capita than Poland [13], which is consistent with the economic motive indicated by respondents in this study, but also countries located close to Poland, which may be related to the fact that respondents may be considering regular visits to Poland.
Most of the migrating respondents (79/102 nurses and 36/60 doctors) indicated economic issues as the main reason for leaving Poland. The second most common response was the issue related to the ineffective organisation of the health care system in Poland – a too wide scope of duties or a too narrow scope of rights, poor working environment, lack of professional opportunities, etc. These factors are well described in the scientific literature [14, 15].
Most of the non-migrating respondents (253/595 nurses and 141/314 doctors) indicated factors related to broadly understood obligations to the family as the main reason to stay in Poland. These reasons were related to the necessity to care for the sick, elderly or a disabled family member. These results are a surprise for us, as we thought that the lack of language knowledge would be the main reason for staying in Poland. However, it turned out that this response was given by only 7% of nurses and 2% of doctors (percentage of non-migrating respondents).
The second most common response was the issue related to advanced age – e.g. close to retirement age, otherwise I would have seriously considered emigration. This respondent’s answer shows why the migration of doctors and nurses, which is assessed as low in Poland [16], is so dangerous for the country as a whole – it is about the generation gap. Migration in this context is very important because the medical staff is aging. The average age of nurses in Poland in 2014 was 49 years [17]. The demographic changes affecting the whole of Europe [3] are leading to the phenomenon of an increasing proportion of elderly in relation to young people starting their professional careers. These young people are very valuable because their loss abroad deepens the generation gap, which at the moment of retirement of the generation of baby boomers [7] will cause a human resource crisis in health care in Poland. The Polish generation gap is mentioned in the Supreme Audit Office publication [18].
Statistical analysis of the research data established that only that people who have worked abroad before and those who have participated in the meetings of the recruitment companies are willing to declare their departure from Poland for work purposes. From a logical point of view, this conclusion is obvious. If someone has confirmed that working abroad is financially rewarding and this person can cope in the new language environment and society, it is clear that this person will be more willing to go there again.
We still do not know why the studied nurses and doctors declare their willingness to work abroad. The statistical analysis did not find any association between the decision to migrate and the net income in household per family member. However, migrants indicated economic reasons as the main reason for leaving Poland. Therefore, more research is needed into the causes of the mobility of the population of Polish nurses and doctors, perhaps using a different methodology.
The limitation of this study is the response rate of 50%. However, it is widely recognised that receiving high response rates in studies of healthcare workers is a huge challenge [19, 20]. Secondly, this study was conducted at one point in time; it would be worth performing the study on the same respondents over time (longitudinal study) to ascertain the real migration scale among respondents. Thirdly, this study included only one city, and in principle a part of this city, so the results could not be generalised. Moreover, the sampling approach does not allow for the generalisation of the results. Sample selection was performed on the basis of respondent availability. The study was conducted with nurses available at a given time and place. The selected study method allowed investigators to obtain a sample with characteristics of a representative sample, since it consisted of various categories of respondents. One essential feature of the sample in this large quantitative study is its size. More than 1,000 participated in the study; hence reliable material for statistical comparisons was obtained and the risk of the effect of extreme cases on the mean scores was minimised.
In conclusion, in view of the limitations outlined above, this study constitutes an important step in the research on the international mobility of medical workers in Poland. Problems of the Polish health care system concerning the aging of the Polish society and the generation gap among Polish doctors and nurses will be a huge challenge for policy makers in Poland. Therefore, the migration of the young generation of nurses and doctors from Poland should become a key element of the human resources policy in Polish health care right now. The statistical analysis did not show that the economic factor was related to the decision to migrate, although qualitative assessment of the responses pointed to economic considerations as the main reason for migration. To summarise the statistical analysis, it can be said that for the studied physicians, the factor most increasing the likelihood was prior work abroad, followed by participation in meetings of recruitment companies. However, in the case of the studied nurses, it was the opposite; the factor that most increased the likelihood of a decision to migrate was participation in the information meetings of recruitment companies, followed by prior work abroad. The longer the work experience among respondents was, the lower was the likelihood of considering the decision to migrate.