A 72-year-old male patient was admitted to the emergency department on January 29, 2018, due to recurrent hypokalemia and fatigue for over 2 years, with exacerbation within the past 3 days. Biochemical parameters showed that serum potassium was 2.08 mmol/l (K 3.5–5.5 mmol/l) and creatine kinase was 9415.1 IU/l (CK 25–190 IU/l). Urinalysis indicated positive urine occult blood, but the red blood cell count in the urine was negative. Serum potassium increased to 2.51 mmol/l after potassium supplementation on January 30, and the CK levels continued to rise to 15800.0 IU/l.
The patient was subsequently admitted to identify the cause of hypokalemia and seek further treatment. The patient had a 2-year history of hypertension without a family history of hypokalemia and hypertension, and blood pressure was controlled at around 140/90 mm Hg through nifedipine controlled-release tablets (30 mg qd). After admission, the patient received a large amount of fluid replacement to prevent acute kidney injury caused by myoglobinuria, and a large dose of potassium supplementation was administered via intravenous and oral methods. On the second day, the serum potassium level increased to 3.11 mmol/l, and the CK level rose to 26393.0 IU/L. On the third day, the CK level dropped to 11717.0 U/l, and all other laboratory tests were normal, including 24-hour urine potassium, blood aldosterone, thyroid function, and antinuclear antibody spectrum. The laboratory tests conducted on the patient after admission are shown in Table I. After excluding most of the potential causes of hypokalemia, the patient was found to have a 2-year history of chewing natural licorice purchased from a pharmacy (20–25 g/day). Therefore, the severe hypokalemic rhabdomyolysis was considered to be induced by licorice consumption.
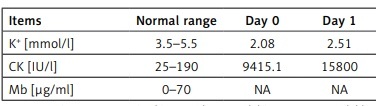
Table I
Partial laboratory tests conducted on the patient after admission
| Items | Normal range | Day 0 | Day 1 | Day 2 | Day 3 | Day 5 | Day 8 |
|---|---|---|---|---|---|---|---|
| K+ [mmol/l] | 3.5–5.5 | 2.08 | 2.51 | 3.11 | 3.24 | 3.65 | 3.44 |
| CK [IU/l] | 25–190 | 9415.1 | 15800 | 26393 | 11717 | 3193 | 424 |
| Mb [µg/ml] | 0–70 | NA | NA | 1321.4 | 1170.4 | 246.4 | 95.3 |
The patient’s biochemical tests subsequently normalized and fatigue subsided. The urinary occult blood also turned negative, with the previous abnormality attributed to myoglobin.
The patient permanently stopped using licorice and its preparations and was followed up for 4 years, without observed hypokalemia or fatigue. Blood pressure has significantly decreased, and can be controlled at around 130/90 mm Hg without antihypertensive drugs.
Licorice, one of the oldest herbal medicines in the world, possesses a wide range of pharmacological effects, including anti-inflammatory, antibacterial, antiviral, and antitumor properties [1]. It is commonly used not only as a medicinal herb but also as a health food product and natural sweetener, due to the concept of “medicine food homology” [2]. However, the potential side effects of licorice are often overlooked or not recognized. The main ingredient in licorice, glycyrrhizin, has been found to inhibit the activity of 11-β-hydroxysteroid dehydrogenase type 2 (11-βHSD2). This enzyme is responsible for converting cortisol to its inactive form, cortisone, and regulating corticosteroid specificity. The inhibitory effects of glycyrrhizin on 11-βHSD2 result in the activation of mineralocorticoid receptors by cortisol, leading to the accumulation of glucocorticoids with anti-inflammatory and mineralocorticoid properties. This can subsequently cause severe hypokalemia and mineralocorticoid-related hypertension [3]. The patient had been chronically taking an excessive amount of licorice, which led to manifestations of pseudohyperaldosteronism, such as hypertension and hypokalemia, through the aforementioned mechanisms. Severe hypokalemia could result in rhabdomyolysis, causing a series of life-threatening syndromes. The toxicity of licorice is related to its dosage. The Chinese Pharmacopoeia stipulates that the prescription dosage of licorice should not exceed 10 g/day; the European Food Safety Authority (EFSA) recommends a daily limit of 100 mg/day for glycyrrhizic acid. One should be vigilant for adverse reactions associated with licorice if symptoms such as edema, dizziness, fatigue, or increased blood pressure occur [4].
In cases of severe hypokalemic rhabdomyolysis with unknown causes, it is crucial for physicians to pay close attention to the patient’s history of licorice consumption. Additionally, testing the plasma concentration of glycyrrhizin can be a useful diagnostic and treatment approach for identifying and managing the side effects of licorice. Lastly, enhancing supervision and education regarding licorice usage may be an effective method to prevent or minimize the occurrence of its side effects.