Introduction
Diabetic mellitus erectile dysfunction (DMED) refers to erectile dysfunction (ED) that is secondary to diabetes. It is distinguished by prolonged or frequent erection and lack of hardness or time to be satisfied [1]. This condition is a form of sexual impairment caused by diabetes [2].
ED is a common and problematic diabetes mellitus complication. The incidence, frequency, and development rate of ED relative to nondiabetic males have been found to be increased in diabetic individuals [3]. In total, 51.3% of diabetic men have self-reported symptoms of ED [4]. They are three times as likely to develop ED as nondiabetic men of similar age [3], and they experience ED onset about 10–15 years earlier than men with erection difficulties due to other causes [3, 5].
Other studies have shown a strong link between ED in men with diabetes and a range of adverse psychosocial outcomes, including reduced quality of life and increased depression, compared to similarly aged men with normal sexual function [3, 6].
Several therapies – both noninvasive and invasive – are available for ED. Today, the first-line intervention for ED is phosphodiesterase type-5 inhibitors (PDE5i). However, PDE5i are successful in only ~60% of patients [7, 8]. In addition, diabetic patients benefit less than patients who are not diabetic [8, 9]. PDE5i are related to adverse events such as headache, flushing, and dyspepsia. The use of PDE5i agents also has a high cost [10, 11].
Alternative ED treatments include intracavernous (ICI) vasogenic injections, prostaglandin E1 intraurethral pharmacotherapy, vascular surgery, and penile prosthesis surgical implantation. Yet, because of their invasive nature and other negatives, none of these treatment options are first-line treatments [7, 12].
Medical care addresses only the complications of ED and does not change the underlying disease pathophysiology. The philosophy of penile rehabilitation is based on the assumption that the erectile system will ultimately be re-established and men will recover spontaneously [13].
Extracorporeal shockwave therapy (ESWT) is a newly developed treatment for ED, using acoustic waves to apply temporary mechanical forces on tissue, which lead to physiological changes such as angiogenesis and neovascularization [14, 15]. Many clinical trials have shown that ESWT is well handled and has good clinical effectiveness in ED care [16, 17]. Physical exercise is also a conservative (alternative) form of ED therapy [18]. Physical exercise is an inexpensive and low-risk technique which can be used with or before pharmacological interventions. Its impact against ED in men is considered to be protective. Exercise reduces the symptoms for people already suffering from ED and protects the general public against ED [19–24]. Further, exercise decreases the risk of reported ED-related cardiometabolism. Thus, there is clear evidence that regular PE significantly increases erectile function. The relationship between PE and ED has been evaluated in previous studies [25–28].
To date, no clinical research has directly evaluated the therapeutic efficacy of ED-management by ESWT in combination with PE. We believed that both interventions would be helpful in the treatment of ED and that the direct comparison of the efficacy of both methods would provide insight into the potential decision-making processes for clinicians and patients regarding alternative therapies with medication or invasive treatments. Therefore, in this randomized clinical trial we carried out a comparative study between the efficiencies of ESWT, PE, and a combination of both in the management of ED.
Material and methods
Subjects
Between September 2019 and October 2020, 45 T2D patients with ED were recruited from the Department of Endocrinology of Cairo University hospitals. Prior to all examinations and interventions, all patients signed written informed consent. The study protocol was approved by the faculty of the physical therapy ethical committee.
Inclusion criteria
Patients who had ED for over 6 months, were 40 to 60 years of age, had type 2 diabetes, had average ratings of over 12 on the International Index of Erectile Function (IIEF-5) five-item edition, had failed or had unsatisfactory results with oral PDE5 inhibitors, were in a committed (married) relationship, and engaged in regular sexual activity for a minimum of 6 months before the study.
Exclusion criteria
Subjects who had any of the following conditions were excluded from enrollment: Severe ED patients (score IIEF-5 < 12), coagulopathy history or recent antiplatelet therapy history, pelvic radiation previously administered, trauma, penile anomalies, prior prostatic surgery, history of malignancy in the last 5 years, unstable spinal cord injury, psychiatric illness, cardiovascular diseases, hypertension with blood pressure > 160/100 mm Hg, smoker, alcoholic or recent anti-androgen or androgen administration. Patients were also excluded if, in the previous 7 days, ED therapy involving oral medicine, VED, ICI, or intraurethral therapy was offered. Men were invited to take part in the secondary study of sexual dysfunction at these sites.
Measurements
Research personnel were offered systematic instruction and qualification in the research procedures performed for all measurements at the baseline before randomization. All subjects were examined properly, and all medical observations and histories were documented. Body mass index (BMI) was measured as weight of the body (in kg) divided by the square height (in cm). Duration of DM, smoking history, and the use of medicines for hypertension and lipid reduction were recorded. The endocrinology department at the hospital had approved the type 2 DM diagnosis. The most recent level of glycated hemoglobin (HbA1c) was documented.
Sexual function
Sexual function was assessed by physical examination and history of sexual activity, using the Arabic version of the International Index of Erectile Function (IIEF-5) as a diagnostic tool [29]. In a single session, all patients completed the IIEF-5 Arabic version without assistance. IIEF-5 is among the most frequently used, validated, and reliable tests for male sexual function [30]. It evaluates the clinical severity of ED within the past 6 months.
The IIEF score ranges between 1 and 25; a score < 22 indicates ED. The severity of ED was evaluated according to the total IIEF score; a score of 1–7 indicates severe ED, a score of 8–11 indicates moderate ED, a score of 12–21 indicates mild ED, and a score of 22–25 indicates no ED.
The evaluation was carried out among all patients at baseline, after 4 weeks, and after 12 weeks of interventions.
Intervention
The patients were randomly assigned to 3 parallel groups: an ESWT group (to undergo ESWT intervention), a PE group (to receive physical exercise treatment), and a combined group (to receive ESWT treatment alongside physical exercise). A random number generator in SPSS 25 for Windows (IBM Corp., Armonk, NY, USA) generated the randomization sequence. The random allocation sequence was implemented using sequentially numerated, unmarked, sealed envelopes. The authors of the study developed the sequence of random allocations, engaged participants, and assigned participants to interventions. However, neither patients nor the clinicians were blinded to the after-assignment procedures.
ESWT group
Patients in the ESWT group were treated through the administration of shockwave therapy technology (Shockmaster MP200, pneumatic-mechanical radial shockwave unit, Storz Medical, Switzerland). With no local or systemic analgesia, ESWT was applied with ultrasound gel. All patients were treated twice per week for 6 weeks, with 3000 shockwaves being administered to the distal penis (1000 shockwaves), penis base (1000 shockwaves), and perineum corporeal bodies (500 shockwaves to each crus). The treatment location and the device’s probe were cleaned and disinfected before and after application to prevent infection. Each patient was required to remove any hair in the application area, 2 days before therapy began. To reduce the risk of injury, shockwaves were not delivered to the testes, spermatic cords, or urethra. With both corpora reaching the depth of the shockwaves, treatment was provided on only one side of the penile shaft. The 3000 shocks were administered according to the manufacturer’s instructions at an energy density of 0.25 mJ/mm2 and an emission frequency of 6 Hz per treatment session, which lasted 15 min. Every patient treated for 6 weeks with ESWT then continued to be followed up for 12 weeks.
PE group
In the PE group, patients were treated with physical exercise. The patients completed an exercise regimen that included 20 min of aerobic exercise accompanied by 10 min of full-body stretching, 30 min of strength exercise, and 10 min of aerobic exercise. To optimize the impact of exercise on recovery, this training program was administered 3 days a week. The patients spent 12 weeks carrying out this program.
Combined group
Patients in the combined group were handled with the same guidelines and procedures as those of the ESWT group using physical activity in the form of the program used by the PE group plus ESWT. To avoid exhaustion, the patients were treated with ESWT on the days when they were not engaging in exercises. ESWT was conducted with exercise for 6 weeks; then ESWT was discontinued and exercise resumed for 12 weeks.
Results
Sample size
The pre-study sample size calculation was performed using G*POWER statistical software [F tests- ANOVA: repeated measurements, between variables, α = 0.05, power = 80%, and large effect size] and revealed that N = 45 was the acceptable sample size for this analysis.
Statistical analysis
Descriptive statistics and an ANOVA test for comparison of the average age of the 3 groups were performed. Data distribution was tested using the Shapiro-Wilk test. To test the homogeneity between groups, Levene’s test for homogeneity of variances was carried out. A mixed MANOVA was conducted to compare the time effect (pre, post I, and post II) and treatment effect (between groups), as well as the relationship between therapy and time on mean IIEF values. For subsequent multiple comparisons, post-hoc tests were performed using the Bonferroni correction. The significance level was set to p < 0.05 for all statistical tests. IBM SPSS version 25 for Windows (IBM Corp., Armonk, NY, USA) provided all statistical tests.
Participant characteristics
Table I displays the characteristics of the participants from groups A, B, and C. The age gap between the three groups (p > 0.05) was not significant.
Effect of treatment on IIEF
A mixed MANOVA showed that therapy and time correlations were significant (F = 49.48, p = 0.001). The main effect of time (F = 408.48, p = 0.001) was significant and the main effect of treatment was significant (F = 17.85, p = 0.001).
Within-group comparison
At post I and post II, there was a significant increase in IIEF compared to pretreatment in the three groups (p < 0.001). In group A, there was a significant decrease in IIEF at post II compared to post I (p < 0.01). In group B, there was a significant increase in IIEF at post II compared to post I (p < 0.001). In group C, there was a significant increase in IIEF at post II compared to post I (p < 0.001).
Between-group comparison
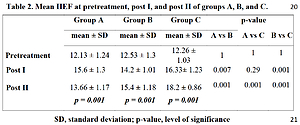
There was no significant difference between the pretreatment groups in IIEF (p > 0.05). Comparison between post I groups showed a significantly higher value in group A IIEF versus group B (p = 0.007) and a significantly higher value in group C IIEF versus group B (p = 0.001). However, the difference between groups A and C (p = 0.29) was not significant. In the post II group C, IIEF was significantly higher compared to groups A and B (p = 0.001) while in group B, IIEF was significantly higher compared to group A (p = 0.001) (Table II).
Table II
Mean IIEF at pretreatment, post I, and post II of groups A, B, and C
Discussion
In modern society, ED is a common disorder in males and directly impacts the consistency of a couple’s sex life. In diabetic patients, the etiology of ED is multifactorial [31]. The mechanisms suggested include neuropathy, vasculopathy, resistance to insulin, visceral adiposity, and hypogonadism. Microvascular dysfunctions are accountable for peripheral circulatory ischemic damage [31]. In addition, both somatic and autonomic neuropathies may lead to DM-induced ED due to the loss of sensory impulses from the penis to the reflexogenic erectile center and the markedly reduced parasympathetic activity essential for relaxation of the corpus cavernous smooth muscle [31]. Men with DM appear to have more serious ED and all of the PDE5Is in this clinical scenario are less successful. PDE5i agents are somewhat recognized as ED first-line therapy [32].
These drugs, however, are not beneficial in all patients, especially those with diabetes-induced ED. Medical treatment addresses only the symptom of ED and does not improve the underlying pathophysiology of the disease mechanism. Penile rehabilitation philosophy is built on the concept that such therapy would ultimately recover the erectile system and enable men to recover spontaneous erection. To our knowledge, this is the first research into the effectiveness of the conjunction of ESWT and physical activity in T2DM and ED patients [13].
Our findings show that the combined strategy offers advantages over ESWT or PE alone in terms of mean IIEF-5 score improvement and outcome durability. The key finding of this study is that treatment of ED in T2DM patients with either ESWT, PE, or both led to significant changes in the IIEF-5 score at 4 and 12 weeks after completion of therapy (as compared to the baseline). In addition, PE and ESWT had comparable efficiencies.
The percentages of progress in the ESWT group were 28% and 12.6%, while the percentages in the PE group were 13% and 22.9%, and the percentages in the ESWT and PE combined group were 33.1% and 48.4% after 4 and 12 weeks, respectively. This showed that in the ESWT and combined groups, the percentage change after 4 weeks was higher than that in the PE alone group, meaning the response to ESWT is faster than the response to PE. There was a decline in the improvement of the ESWT group after 12 weeks, but there was an increase in the PE group and the combined group after 4 weeks as opposed to the measurement. This means that ESWT’s durability alone is less than the durability of the PE and ESWT combinations. No pain or side effects connect the shockwave energy and exercise treatment used in the present research.
ESWT has been widely used to treat various disorders, including urolithiasis [33], chronic damage to the motor system, and Peyronie’s disease [34]. A shockwave is a form of high-energy mechanical acoustic wave that yields a pressure impulse as it spreads through a medium. The waves can be non-invasively modified, allowing for the delivery of a controllable amount of energy at the desired location. The concentrated waves interact with selected deep tissues, inducing several biological changes, including weakening fibrous adhesions, stimulating capillary formation, and promoting hyperplasia of the vascular endothelial cells [14]. Several controlled clinical trials in recent years have shown ESWT’s beneficial effects in patients with physical ED [14–18].
The underlying mechanisms of ESWT’s positive impact still hard to be fully explained, although some animal studies have elucidated that. ESWT has been shown to considerably boost the erectile capacity of diabetic rats and to contribute to the growth of smooth muscle and endothelial cells [35], and, thus, to elicit a time- and treatment-dependent reduction in the ratio of intracavernosal pressure to mean arterial pressure, likely due to apoptosis and collagenisation of smooth corporal muscle [36].
Research using molecular biology techniques has shown that ESWT upregulated the α-smooth muscle actin, von Willebrand factor, neuronal NO synthase, and vascular endothelial growth factor expression and downregulated the receptor’s expression for advanced glycation end products in the corpus cavernosum [37]. We believe that ESWT enhances erectile function through a variety of measures, which include eliminating fibrosis and apoptosis, improving microcirculatory blood flow in local tissue, and releasing tissue factors such as endothelium-derived relaxing factor and various growth factors.
ESWT’s proposed mechanisms of action in ED patients may reflect the reasoning behind the consistency of the findings reported in patients undertaking the combined approach. Admittedly, energy from ESWT’s acoustic waves has been proposed to stimulate cellular and molecular pathways, increasing the production of local growth factors and enhancing endothelial activity, angiogenesis, and nerve fiber regeneration. ESWT therefore has the ability to recover normal erections and treat the disease [38].
Penile erection is a physiologic mechanism involving increased arterial inflow and venous outflow limits [19]. Endothelial inflammation which interferes with the production of nitric oxide (NO) is a key element of vascular diseases, particularly ED [39]. Neuronal and endothelial NO mediate the vascular portion of sexual excitement by engorgement of the corpora cavernosa tissue and subsequent penile erection. It is well understood that the erectile flow of blood is controlled by the smooth muscle cells of penile arterial vessels being constricted or relaxed [40]. Physical exercise (PE) may eventually lower ED, and PE has been established as the lifestyle factor most strongly associated with erectile function, in addition to being the most significant vascular health promoter. Therefore, moderate- and vigorous-intensity PA is correlated with healthy erectile function and lower ED risk [19–22].
PE induces endothelial function and NO development and has been consistently demonstrated to enhance erectile function. PE also increases erectile function by inducing a rise in serum total testosterone in males. Hence, there is good evidence that regular PE considerably increases erectile function [27].
First, while both ESWT or PE alone and the combined model involving ESWT and PE produced statistically significant changes in the mean IIEF-5 ratings, the degree of difference reported in patients receiving the latter modality of care was significantly higher in patients receiving the combined approach of ESWT and PE in the 4- and 12-week follow-ups. Durability following treatment with ED remains largely under-investigated. In addition, we verified PE’s durability alone or the combined approach, even at the 12-week follow-up.
Interestingly, a deterioration was noticeable in patients receiving ESWT alone at the 12-week follow-up, while efficacy remained stable in patients receiving PE or the combination treatment.
Based on the findings of this research, patients with diabetic ED should be advised on the possible benefits offered by a combination approach involving ESWT and PE in terms of enhancing the clinical effectiveness of IIEF-5 and its durability.
In our present research, we recognize the various limitations, such as the lack of a placebo (control) arm, objective penile hemodynamic measurements, the limited number of participants, and the short-term follow-up. We believe that even more basic research is needed to explore the different pathophysiological mechanisms of combining ESWT with PE in relation to erectile tissue including long-term effectiveness, safety, and histological changes.
Although current findings appear promising, several main factors related to ESWT and PE, such as shockwave energy, physical activity, shockwave treatment models and protocols, patient characteristics, actual physiological changes in penile tissue, and long-term effectiveness and protection, have yet to be completely investigated.
In conclusion, both ESWT and PE significantly improve the management of ED in diabetic patients, though the combined approach of ESWT and PE provides significant advantages in erectile dysfunction improvement and durability as compared to ESWT or PE alone in diabetic patients with ED.