Current issue
Archive
Manuscripts accepted
About the Journal
Editorial office
Editorial board
Section Editors
Abstracting and indexing
Subscription
Contact
Ethical standards and procedures
Most read articles
Instructions for authors
Article Processing Charge (APC)
Regulations of paying article processing charge (APC)
PULMONOLOGY / RESEARCH PAPER
Demarcated by bronchial or vascular landmarks? a study on the lower borders of the lower paratracheal lymph nodes
1
Department of Respiratory and Critical Care Medicine,the Second Hospital Affiliated to Nanjing Medical University, China
2
Radiology department,the Second Hospital Affiliated to Nanjing Medical University, China
3
Department of thoracic surgery,the Second Hospital Affiliated to Nanjing Medical University, China
4
Department of Respiratory and Critical Care Medicine, Second Affiliated Hospital Zhejiang University School of Medicine,Hangzhou, China, China
Submission date: 2022-08-26
Final revision date: 2023-01-30
Acceptance date: 2023-02-22
Online publication date: 2023-02-26
Corresponding author
Ganzhu Feng
Department of Respiratory and Critical Care Medicine,the Second Hospital Affiliated to Nanjing Medical University, No 121,xiaguan District,Nanjing,Jiangsu, 210011, Nanjing, China
Department of Respiratory and Critical Care Medicine,the Second Hospital Affiliated to Nanjing Medical University, No 121,xiaguan District,Nanjing,Jiangsu, 210011, Nanjing, China
KEYWORDS
TOPICS
ABSTRACT
Introduction:
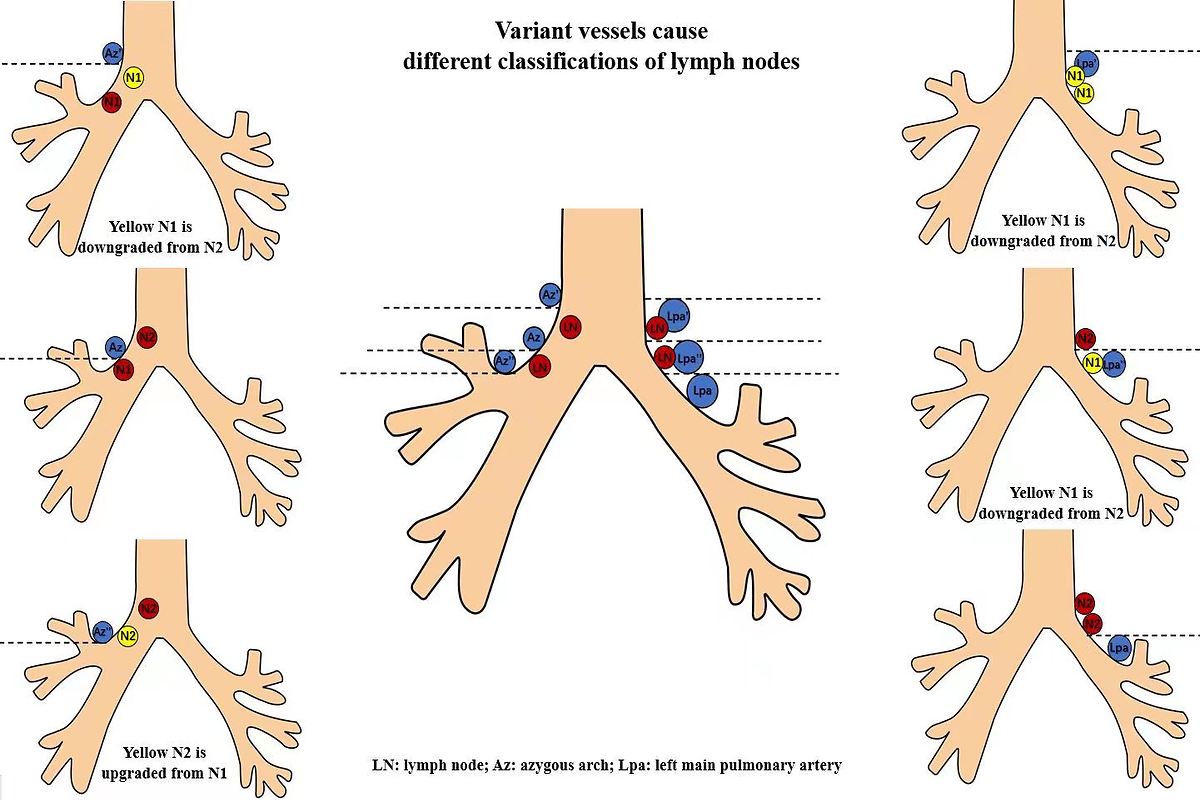
The lower rim of the azygous arch and the upper rim of the left main pulmonary artery are used as the lower borders of the lower paratracheal lymph nodes (LNs) in the IASLC map. However, there is some confusion about it. Our aim was to investigate the best landmarks as the boundaries to stage N more accurately for lung cancer.
Material and methods:
One hundred patients with benign lung diseases, fifty with lung cancer diagnosed by endobronchial ultrasound-guided transbronchial needle aspiration (EBUS-TBNA), and thirteen with right metastatic LNs confirmed by surgery were included. The lymph nodes (including W1, W3, W5, 10R below W5, W4, W6) were classified with Wang's and IASLC map concurrently, and the different outcomes of N stage were compared.
Results:
The azygous arch and the left main pulmonary artery varied in relation to the airway, causing the following changes of classification, 9.4% benign LNs of W1 and 38.6% of W5 were down-regulated as IASLC-10R, 9.5% of 10R below W5 were up-regulated as IASLC-4R, 51.4% of W4 and 94% of W6 were down-regulated as IASLC-10L. In 50 patients diagnosed by EBUS-TBNA, the concordance between the two maps was 0.768 for the right 92 LNs, while it was 0.374 for the left 46 nodes. If based on the location of azygous arches, postoperative stages might be changed in 2 surgery patients.
Conclusions:
The locations of the lower vascular boundaries of IASCL-4 were varied. The bronchial landmarks of the proximal right and left main bronchus might be used as such borders.
The lower rim of the azygous arch and the upper rim of the left main pulmonary artery are used as the lower borders of the lower paratracheal lymph nodes (LNs) in the IASLC map. However, there is some confusion about it. Our aim was to investigate the best landmarks as the boundaries to stage N more accurately for lung cancer.
Material and methods:
One hundred patients with benign lung diseases, fifty with lung cancer diagnosed by endobronchial ultrasound-guided transbronchial needle aspiration (EBUS-TBNA), and thirteen with right metastatic LNs confirmed by surgery were included. The lymph nodes (including W1, W3, W5, 10R below W5, W4, W6) were classified with Wang's and IASLC map concurrently, and the different outcomes of N stage were compared.
Results:
The azygous arch and the left main pulmonary artery varied in relation to the airway, causing the following changes of classification, 9.4% benign LNs of W1 and 38.6% of W5 were down-regulated as IASLC-10R, 9.5% of 10R below W5 were up-regulated as IASLC-4R, 51.4% of W4 and 94% of W6 were down-regulated as IASLC-10L. In 50 patients diagnosed by EBUS-TBNA, the concordance between the two maps was 0.768 for the right 92 LNs, while it was 0.374 for the left 46 nodes. If based on the location of azygous arches, postoperative stages might be changed in 2 surgery patients.
Conclusions:
The locations of the lower vascular boundaries of IASCL-4 were varied. The bronchial landmarks of the proximal right and left main bronchus might be used as such borders.
Share
RELATED ARTICLE
| eISSN: | 1896-9151 |
| ISSN: | 1734-1922 |
We process personal data collected when visiting the website. The function of obtaining information about users and their behavior is carried out by voluntarily entered information in forms and saving cookies in end devices. Data, including cookies, are used to provide services, improve the user experience and to analyze the traffic in accordance with the Privacy policy. Data are also collected and processed by Google Analytics tool (more).
You can change cookies settings in your browser. Restricted use of cookies in the browser configuration may affect some functionalities of the website.
You can change cookies settings in your browser. Restricted use of cookies in the browser configuration may affect some functionalities of the website.