Introduction
The 2020 global cancer burden data show that tracheal, bronchial, and lung (TBL) cancer is the second most prevalent cancer in the world after female breast cancer [1]. Despite all this, TBL cancer continued to be the leading cause of cancer death in 2020, accounting for 1.8 million deaths globally [1]. However, the main causes of cancer deaths vary greatly among countries and among regions within each country and are considered to be closely linked to economic development and related social and lifestyle factors [2].
The etiology of TBL cancer involves multiple factors, including genetic and environmental factors. Among these, smoking, ambient particulate matter pollution, secondhand smoke, and household air pollution from solid fuels are related to the respiratory system and form the four most important risk factors that contribute to the disability-adjusted life year (DALY) rate of TBL cancer [3]. According to our knowledge, no study has investigated the trends of the changes in age-standardized DALY rates and age-standardized death rates (ASDRs) of TBL cancer attributable to these four risk factors.
Based on data from the 2019 Global Burden of Disease (GBD) study, this study analyzed the disease burden of TBL cancer, in terms of the DALY rate and death rate, attributable to four major risk factors (smoking, ambient particulate matter pollution, secondhand smoke, and household air pollution from solid fuels [3]) in 204 countries and regions from 1990 to 2019 [4, 5]. At the same time, all nations were categorized into five groups based on their Socio-Demographic Index (SDI) scores (low, low-middle, middle, high-middle, and high).
Material and methods
Source of data
The 2019 GBD research provided the data for this investigation. The 2019 GBD study used a unified method to conduct a comprehensive disease burden assessment of 369 diseases and injuries and 87 risk factors in 204 countries and regions around the world [4, 5].
We used DisMod-MR 2.1 to calculate the data indicators and to determine the 95% uncertainty intervals.
According to the International Classification of Diseases, ICD9 codes 162–162.9, 212.2–212.3, 231.1–231.2, and 235.7 and ICD-10 codes C33–C34.9, D02.1–D02.3, D14.2–D14.3, and D38.1, TBL cancer in the GBD study was classified.
Risk factors
In the GBD 2019 study, the mortality and DALYs attributable to 87 risk factors and clusters of risks were estimated at the global and regional levels via six analysis steps and involving 30,652 data sources [5]. The exposure levels were summarized into binary, multiple, and continuous risk factors using aggregated exposure values to facilitate comparison between different times, locations, and risks. Details can be found in other articles [5].
Statistical analysis
The estimated annual percentage changes (EAPCs) in the age-standardized rates (ASRs) of TBL cancer were computed within a predetermined time period using the following two formulas: y = α + βx + ε and EAPC = 100 × (exp(β) − 1). Among them, y refers to ln (ASR), x is the calendar year, ε is the error term, and β represents the positive or negative ASR trends. The formulas were based on the linear relationship between the natural logarithm of ASR and time. 95% confidence intervals (CIs) were determined using the linear model. The ASR trend is upward when the EAPC and CI lower limit are positive. Conversely, the ASR trend is downward when the EAPC and CI upper limit are negative. Otherwise, the ARS exhibits a steady trend [6].
Results
Global disease burden of TBL cancer
From 1990 to 2019, the age-standardized DALY rate and ASDR of TBL cancer attributable to total risk factors exhibited globally a decline trend. Among the individual risk factors, the age-standardized DALY rate (EAPC = 0.60, 95% CI: 0.50 to 0.70) and ASDR (EAPC = 0.91, 95% CI: 0.80 to 1.01) only attributable to ambient particulate matter pollution showed a rising trend (Tables I and II).
Table I
Trends of age-standardized DALY rate of TBL cancer attributable to respiratory system-related risk factors in each region from 1990 to 2019
Table II
Trends of age-standardized death rate of TBL cancer attributable to respiratory system-related risk factors in each region from 1990 to 2019
Disease burden of TBL cancer by SDI regions
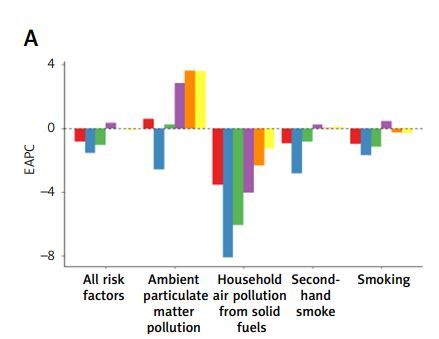
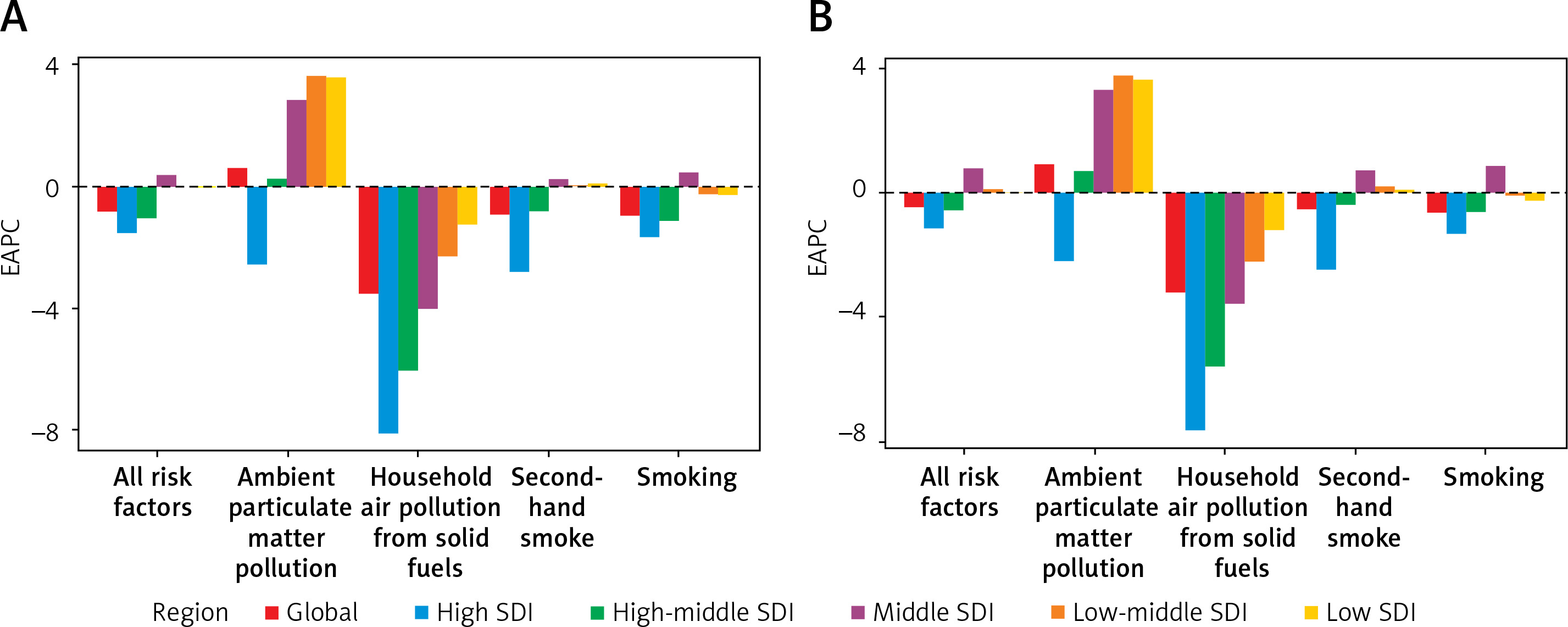
The age-standardized DALY rate and ASDR of TBL cancer attributable to total risk and smoking exhibited an upward trend in the middle SDI region, those attributable to ambient particulate matter pollution only decreased in the high SDI region, those attributable to secondhand smoke decreased in the high and high-middle regions, those attributable to household air pollution from solid fuels decreased in all five SDI regions, and the decline in the ASR elevated with increasing SDI (Tables I and II, Figures 1 A and B).
Disease burden of TBL cancer attributable to total risk factors
At the regional level, except in East Asia, Western Sub-Saharan Africa, Oceania, and North Africa and the Middle East (EAPC = 0.44, 0.40, 0.24, and 0.01, respectively), the age-standardized DALY rates exhibited a downward trend, especially in Eastern Europe (Table I). At the national level, Bahrain experienced the greatest decline. However, several countries exhibited a rising trend, including Mozambique, Bulgaria, Lesotho, Honduras, and Lebanon, among which Mozambique shown the greatest growth (EAPC = 1.71, 95% CI: 1.56 to 1.85) (Supplementary Table SI).
Except in East Asia, Western Sub-Saharan Africa, Oceania, and North Africa and the Middle East (EAPC = 0.93, 0.59, 0.27, 0.25, respectively), the ASDRs exhibited a downward trend, especially in Eastern Europe (Table II). The three largest reductions in ASDRs were observed in Bahrain, Kyrgyzstan, and Ukraine. In addition, those in many countries, including Bulgaria, Honduras, and Lebanon (EAPC = 1.91, 1.68, 1.60, respectively), exhibited an upward trend (Supplementary Table SII).
Disease burden of TBL cancer attributable to smoking
The age-standardized DALY rates exhibited the most significant declines in Central Latin America, Australasia, and Eastern Europe. The rates in East Asia (EAPC = 0.65, 95% CI: 0.42 to 0.87) exhibited an upward trend (Table I). Bahrain, Kyrgyzstan, and Singapore saw the biggest drops. Some countries, including São Tomé and Príncipe (EAPC = 1.76, 95% CI: 1.69 to 1.84) and Bulgaria (EAPC = 1.69, 95% CI: 1.18 to 2.20), showed a rising trend (Supplementary Table SI). In 2019, Greenland, Montenegro, and Monaco were the top three countries with the highest rates (Supplementary Figure S1 A). Males aged 70 to 74 and females aged 75 to 79 experienced the highest DALY rates (Supplementary Figure S2 A).
The upward trends in the ASDRs were observed in East Asia, Western Sub-Saharan Africa, North Africa and Middle East, and Oceania (EAPC = 1.10, 0.39, 0.13, 0.01, respectively). The largest decline was observed in Central Latin America (Table II). The largest drops were seen in Bahrain, Mexico, and Singapore, while Bulgaria, São Tomé and Príncipe, and Lebanon (EAPC = 1.90, 1.79, 1.63, respectively) showed the most significant increases (Supplementary Table SII). In 2019, Greenland, Monaco, and Montenegro were the top three countries with the highest rates (Supplementary Figure S1 B). The death rate peaked for men between the ages of 85 and 89, whereas it peaked for women between the ages of 95 and older (Supplementary Figure S2 B).
Disease burden of TBL cancer attributable to ambient particulate matter pollution
Nearly half of the 21 regions exhibited a rising trend in age-standardized DALY rates. The most significant increase in this rate was observed in Western Sub-Saharan Africa (EAPC = 3.65, 95% CI: 3.46 to 3.83). In the remaining 11 regions, the greatest diminution was found in high-income North America (Table I). In that regard, more than half of the countries exhibited a rising trend, with the most significant increases observed in Equatorial Guinea, Bhutan, and Mozambique (EAPC = 9.02, 6.62, 5.63, respectively). The largest decline was found in Finland (Supplementary Table SI). In 2019, Serbia, Montenegro, and China were the top three countries with the highest rates (Supplementary Figure S3 A). The DALY rate was the highest in the 70–74 age range for both sexes (Supplementary Figure S4 A).
The ASDRs in more than half of the regions exhibited a rising trend, with the most significant increases observed in Western Sub-Saharan Africa, East Asia, and Eastern Sub-Saharan Africa (EAPC = 3.89, 3.72, 3.66, respectively). The largest decline was found in high-income North America (Table II). The ASDRs in more than half of the countries increased, with the greatest increase found in Equatorial Guinea (EAPC = 9.55, 95% CI: 8.92 to 10.18). The most significant decrease was observed in Finland (Supplementary Table SII). In 2019, China, Serbia, and Montenegro were the top three countries with the highest rates (Supplementary Figure S3 B). The death rate peaked for men between the ages of 85 and 89, whereas it peaked for women between the ages of 95 and older (Supplementary Figure S4 B).
Disease burden of TBL cancer attributable to secondhand smoke
High-income North America, Australasia, and Andean Latin America were the three regions that exhibited the biggest decreases in age-standardized DALY rates. Western Sub-Saharan Africa, Oceania, South Asia, and East Asia exhibited the rising trends, especially Western Sub-Saharan Africa (EAPC = 0.71, 95% CI: 0.66 to 0.75) (Table I). Mexico, the United States of America, and Singapore showed the largest declines. Notably, the DALY rates increased in more than 60 countries, including Lesotho (EAPC = 2.01, 95% CI: 1.69 to 2.33), and Lebanon (EAPC = 1.95, 95% CI: 1.58 to 2.33) (Supplementary Table SI). In 2019, Montenegro, Greenland, and Hungary were the top three countries with the highest rates (Supplementary Figure S5 A). The rates were the highest in the 70-74 age range for both sexes (Supplementary Figure S6 A).
Except for the four regions of Western Sub-Saharan Africa, East Asia, Oceania, and South Asia, the ASDRs in all other regions showed a declining trend, especially in high-income North America (Table II). Those that showed the greatest declines were Mexico, the United States of America, and Switzerland. The ASDRs increased in some countries, such as Lebanon, Lesotho, Georgia, and Honduras, with the greatest increase found in Lebanon (EAPC = 2.13, 95% CI: 1.72 to 2.54) (Supplementary Table SII). In 2019, Montenegro, Greenland, and Hungary were the top three countries with the highest rates (Supplementary Figure S5 B). The rate peaked for men between the ages of 85 and 89, whereas it peaked for women between the ages of 95 and older (Supplementary Figure S6 B).
Disease burden of TBL cancer attributable to household air pollution from solid fuels
All regions show a downward trend in age-standardized DALY rates. Among them, Australasia, high-income Asia Pacific, and Eastern Europe were the three regions that saw the biggest drops (Table I). The DALY rates decreased in most countries, with the most significant decreases in Saudi Arabia, Libya, and the United Arab Emirates. Notably, the rates increased in seven countries, namely Mozambique, Chad, Lesotho, Zimbabwe, Guinea, Honduras, and Papua New Guinea, with the greatest increase observed in Mozambique (EAPC = 1.16, 95% CI: 1.02 to 1.30) (Supplementary Table SI). In 2019, Solomon Islands, Uzbekistan, and Papua New Guinea were the top three countries with the highest rates (Supplementary Figure S7 A). The rates were the highest in the 70–74 age range for both sexes (Supplementary Figure S8 A).
The ASDRs also exhibited a declining trend in all 21 regions. Australasia, high-income Asia Pacific, and Eastern Europe were the three regions that saw the biggest drops (Table II). The rates decreased in most countries, with the greatest decreases observed in Saudi Arabia, Libya, and the United Arab Emirates. The rates in nine countries, namely Mozambique, Chad, Honduras, Lesotho, Niger, Papua New Guinea, Guinea, Burkina Faso, and Zimbabwe, exhibited a rising trend, with the largest increase found in Mozambique (EAPC = 1.03, 95% CI: 0.91 to 1.15) (Supplementary Table SII). In 2019, Solomon Islands, Vanuatu, and Papua New Guinea were the top three countries with the highest rates (Supplementary Figure S7 B). The rate peaked for men between the ages of 85 and 89, whereas it peaked for women between the ages of 80 and 84 (Supplementary Figure S8 B).
Discussion
The GBD 2019 study conducted a comprehensive survey and summary of TBL cancer worldwide and extensively summarized the risk factors for TBL cancer [3]. It is worth noting that the DALYs and deaths associated with TBL cancer caused by risk factors account for a significant portion of the overall burden of TBL cancer, indicating that prevention and control of the disease burden of TBL cancer linked to risk factors are urgently needed. However, different risk factors have different degrees of impact on the TBL cancer burden in various regions and countries. Therefore, to help formulate more personalized prevention and control policies, we investigated the trends of changes in the disease burden (DALY rate and death rate) of TBL cancer attributable to four major risk factors in 204 countries and 21 regions worldwide from 1990 to 2019. Our research found that during this period, those attributable to total risk factors and four major risk factors all exhibited a decline trend globally. In contrast, those attributable to ambient particulate matter pollution showed a rising trend.
Among all of the SDI regions, the most comprehensive control of TBL cancer was found in high SDI regions. Specifically, the household air pollution from solid fuels had been effectively controlled during this period, which may be related to the high level of overall social economic development, universal coverage of health awareness, people’s increasing attention to their own health, and increasing access to cancer prevention, diagnosis, and comprehensive treatment. Importantly, the control of ambient particulate matter pollution in other SDI regions were especially dismal.
Smoking is recognized as a controllable behavioral risk factor with a major influence on the occurrence and development of TBL cancer. According to some research, the risk of lung cancer drops to around half that of smokers 10 years after quitting [7]. Even later in life, quitting smoking can lower the chance of cancer formation, and for those who have already been diagnosed with lung cancer, quitting smoking can still, to some extent, lower the incidence of early death [8]. The impact of smoking cessation on TBL cancer is self-evident. Among the 21 regions, Central Latin America, Australasia, and Eastern Europe most effectively promoted smoking cessation over the study period and consequently showed the greatest reduction in the burden of TBL cancer. However, the burden of TBL cancer attributable to smoking in East Asia and Western Sub-Saharan Africa increased during this period, highlighting the need to improve relevant policies and strengthen smoking control in these regions.
Environmental particulates, such as fine particulate matter, can penetrate into the lungs and enter the bloodstream, making ambient air pollution a risk factor for lung disease [9, 10]. However, nearly half of the regions and countries failed to effectively control ambient particulate matter pollution in the study period. This was especially evident in Western Sub-Saharan Africa, Eastern Sub-Saharan Africa, East Asia, and South Asia where, compared with other regions, ambient particulate matter pollution significantly increased, mainly owing to contributions by countries such as Equatorial Guinea, Bhutan, Cabo Verde, and Djibouti. The increase in disease burden attributable to that in these four regions may be related to sand and dust transport in desert and arid loess areas, low vegetation coverage, and dense urban construction leading to local induced sand and dust [11]. Noteworthy is the fact that high-income North America saw the largest drops in ASRs, followed by Eastern Europe, and the main contributing countries may be the United States of America and Estonia. This result may be related to the increased emphasis on new energy industries and relevant legal and policy support in these nations. High-income countries and some middle-income countries have enacted relevant laws and regulations for this purpose, based on the polluter-pays principle, and have cleaned up the most serious hazardous waste sites [12]. It is understood that the improvement of air quality not only reduces the number of deaths from cardiovascular and respiratory diseases in high-income countries but also brings significant economic benefits. For example, in the United States of America, since 1970, for every $1 invested in air pollution control, it is estimated that there will be a return of $30 (95% CI: $4–$88) [13]. Although controlling air pollution has a positive impact on health and the economy, the importance of air pollution issues has been largely ignored in some regions and countries, especially low-income and middle-income countries [14, 15]. This may explain why the TBL cancer burden attributable to ambient particulate matter pollution was only found to decrease in high SDI regions, while that in other regions showed a gradual increase with the increase in SDI. Therefore, improving air quality is crucial from both the health and economic perspectives.
According to studies, exposure to secondhand smoking raises cancer development risk by 16% when compared to no exposure [16]. From 1990 to 2019, the disease burden attributable to secondhand smoke exhibited an upward trend in the four regions of Western Sub-Saharan Africa, East Asia, Oceania, and South Asia. Most countries in these four regions belong to less developed regions. Thus, the increased disease burden may be related to poor medical conditions and limited access to good comprehensive care for patients. Similarly, the decline in the disease burden attributable to secondhand smoke was the greatest in high-income North America, possibly due to the significant reduction in household exposure to secondhand smoke caused by the implementation of family smoking bans [17]. In addition to smoking bans in residences, smoking bans are also required in public places, which can greatly reduce exposure to secondhand smoke.
Among the four major risk factors, the disease burden attributable to household air pollution from solid fuels exhibited a declining trend in all regions, especially in Australasia. Notably, the decline in the disease burden attributable to this factor was generally greater than that attributable to other risk factors, especially in Saudi Arabia, Libya, and the United Arab Emirates, with EAPCs > 16–17. On the contrary, the disease burden attributable to this factor showed an upward trend in nine countries, including Mozambique, Chad, and Honduras, all of which belong to the low and low-middle SDI categories with poor economic development. Liquefied petroleum gas has entered thousands of households, but in underdeveloped regions, a large proportion of households still use readily available solid fuels, such as cow dung and wood, as cooking fuel [18].
This study’s primary advantage is that we did a comprehensive review of the changes in the burden of TBL cancer in 204 nations and 21 regions from 1990 to 2019, based on the latest and most comprehensive dataset available globally. This study is the first to analyze the impact of risk factors on the disease burden of TBL cancer in terms of both total and individual risk factors, namely smoking, ambient particulate matter pollution, secondhand smoke, and household air pollution from solid fuels. However, this study also has certain limitations. The data were collected over a span of 20 years, during which period considerable improvements in screening technology and different screening methods across countries may have had an impact on the data. In addition, the registration of TBL cancer cases in some low SDI regions may be incomplete, so GBD data in these regions cannot be guaranteed to be accurate and of high quality. Finally, due to the lack of information on the classification, staging, and treatment of TBL cancer, further analysis of the disease burden and risk factor control are difficult.
In conclusion, the global burden of TBL cancer has changed over the past 20 years, and our study gives a thorough summary of those changes. The changes in ASRs of TBL cancer varied by region, country, and SDI. Overall, from 1990 to 2019, the ASRs of TBL cancer attributable to total risk factors decreased globally. Among the four major risk factors, household air pollution from solid fuels was the best controlled in all regions and almost all countries. The risk factors of smoking and secondhand smoke have received widespread attention in most regions and countries, but the control of smoking has been inadequate in Western Sub-Saharan Africa, East Asia, North Africa and Middle East, and Oceania, while the control of secondhand smoke warrants more efforts in Oceania, Western Sub-Saharan Africa, East Asia, and South Asia. Moreover, the problem of ambient particulate matter pollution remains very serious in regions such as East Asia and Western Sub-Saharan Africa, as well as countries such as Equatorial Guinea and Bhutan, where the death and DALY rates attributable to this risk factor were found to be highest in the 50+-year and 60–79-year age groups, respectively.