Introduction
Asthma is the most common chronic childhood disease in the world. According to the guidelines of the World Health Organization on Integrated Management of Childhood Illness (IMCI), the diagnosis of asthma is based on the presence of wheezing [1–3]. It is closely associated with childhood asthma and bronchiolitis. Cough variant asthma (CVA) mainly has features such as repeated episodes of coughing and prolonged treatment [4–6]. Long term irritant dry cough, less sputum and other severe symptoms may occur when cold irritation or pollen allergens gain access. Cough variant asthma is a special type of asthma and chronic cough (cough lasts for more than 8 weeks and chest X-ray shows no evidence of lung disease) is a main manifestation. In children with CVA, IgM antibody level, serum total IgE level and peripheral eosinophil count should be determined to rule out Mycoplasma pneumoniae. In a study based on 10 000 samples, the highest age of developing CVA among children is 3–6 years, the ratio of incidence between boys and girls is 1.42 : 1 and CVA accounts for 14–33% of the causes of chronic cough [1].
In low-income countries, pneumonia is considered to be the main cause of respiratory disease and death among children under 5 years of age [7, 8]. Mycoplasma pneumoniae is a pathogenic microorganism, which is mainly adsorbed on the surface of the airway mucous membrane [9–11]. It destroys the secretion of airway epithelial cells and glands, inhibiting cilium movement and so on. This can cause chronic inflammatory changes in the respiratory system. After long-term mycoplasma pneumonia, the airway smooth muscle becomes contracted, leading to dysfunction of non-cholinergic nerves, airway responsiveness, exacerbating inflammation and migrating disease [11].
The relationship between Mycoplasma pneumoniae infection and asthma has become a hot topic. Because of genetic differences among individuals, chronic and nonspecific airway inflammation leads to edema of the airway mucous membrane, increased mucus secretion and spasm of bronchial smooth muscles. Further studies on the etiology and determinants of asthma suggest that Mycoplasma pneumoniae is one of the pathogens associated with acute or chronic asthma [10].
Since the association between CVA and Mycoplasma pneumoniae still needs to be analyzed, an exploration of the relationship was conducted. This study aimed to analyze the relationship between CVA and Mycoplasma pneumoniae infection in children.
Material and methods
Search strategy
The main aim of this study was to evaluate the relationship between CVA and Mycoplasma pneumoniae. To identify all of the relevant publications, multiple electronic databases including PubMed, Springer, EMBASE, OVID and China Journal Full-text Database were searched, without language restrictions. To increase search accuracy, the following MeSH (Medical Subject Headings) terms were assembled with the Boolean operator “AND”: (1) Cough variant asthma OR CVA; (2) Mycoplasma pneumoniae OR MP; (3) Child OR Children. Related articles with all publication statuses (published, unpublished, in press and in progress) published from January 2000 to January 2020 were systematically searched and reviewed. Two authors in our team searched the literature independently and examined the reference lists to obtain additional relevant studies that were not identified.
Study selection
Two authors selected the citations independently in this study with the following inclusion criteria: (1) pediatric patients with CVA; (2) sample size more than 10; (3) randomized controlled trial or controlled clinical trial; (4) availability of full text; (5) since clinical laboratories can provide diagnostic testing for Mycoplasma pneumoniae infections using culture, serology, or nucleic acid amplification methods, blood test results should be reported. The exclusion criteria were: (1) patients without CVA or adult patients; (2) sample size was less than 10; (3) case report or meta-analysis; (4) results about patients were ineligible. They screened the titles and abstracts of the articles identified, and subsequently, the full text of the studies that potentially met the criteria was obtained. These two investigators determined the included articles together, and disagreements were resolved by consultation with a third investigator if necessary.
Data extraction
After reading the full text of the articles, we extracted the characteristics from each study using a standard data extraction method: the first author’s name, year of publication, nation, age range of patients, sex (male/female), sample size (cough variant asthma (CVA)/simple cough (SC)), follow-up duration, and other parameters. SC patients only had cough without other symptoms.
Statistical analysis
The meta-analyses were conducted with the software Review Manager 5.2 (The Cochrane Collaboration, 2011) to estimate the association between cough variant asthma and Mycoplasma pneumoniae in child patients. For continuous outcomes, standard mean difference (SMD) with 95% confidence interval (CI) was calculated. For discontinuous outcomes, odds ratio (OR) with 95% CI was conducted. A p-value < 0.05 was considered to be statistically significant. Heterogeneities in this study were assessed using the I2 index. We chose the random-effects model when the heterogeneity I2 statistic was > 50%; otherwise, the fixed-effects model was applied.
In addition, the quality of the studies was assessed with sensitivity analysis and bias analysis. The risk of bias table of the included studies was independently assessed according to the Cochrane Handbook for Systematic Reviews of Interventions by two members of our team. In addition, if there was poor agreement and no consensus could be achieved, a third investigator was the adjudicator.
Results
Search results
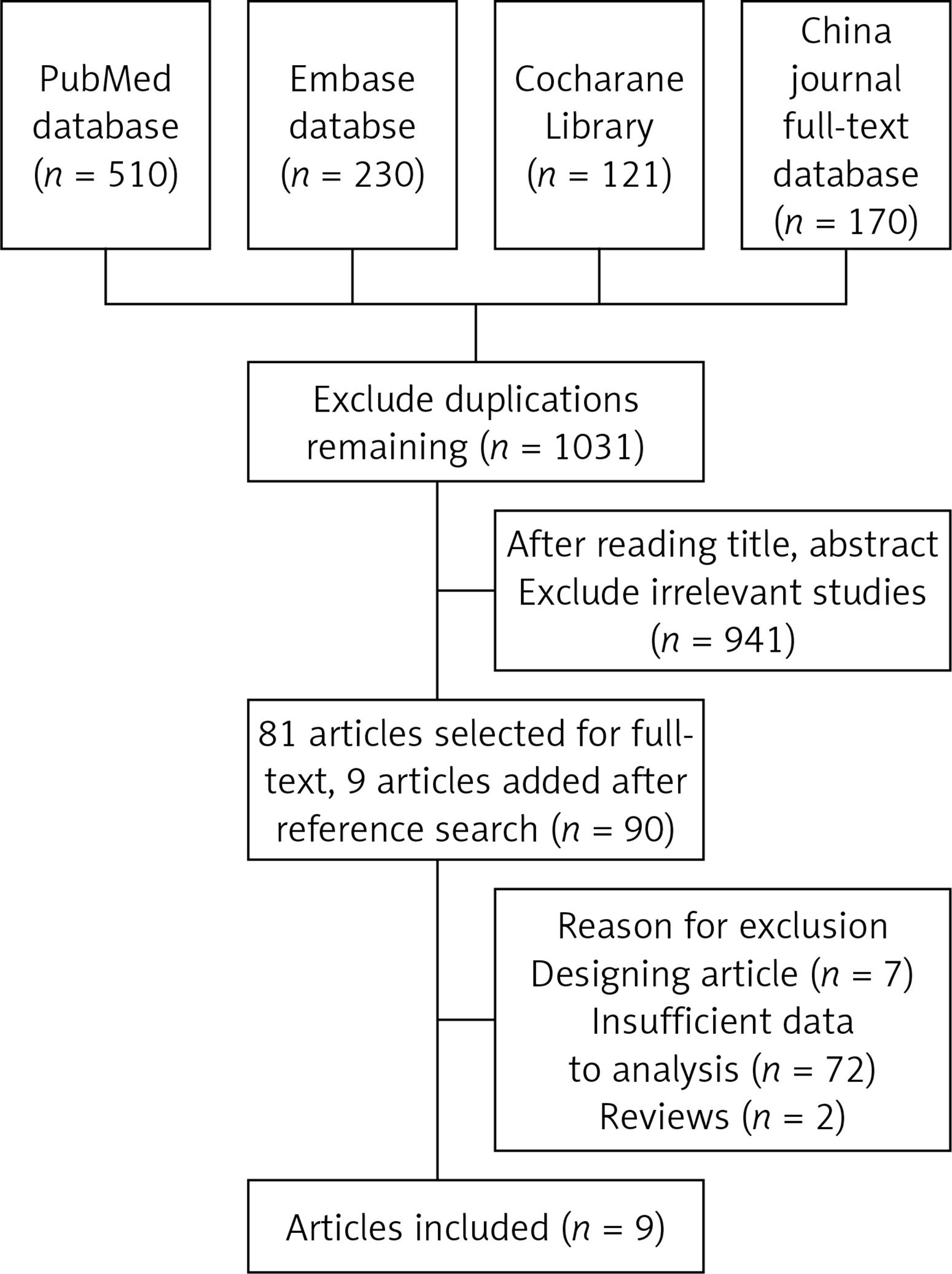
As shown in the flow diagram (Figure 1), 1031 relevant studies were initially identified, and 1022 articles were excluded due to duplication, irrelevant studies, incomplete data, incomplete comparison, other diseases and lack of the full text. Finally, 9 articles [12–20] satisfied the inclusion criteria. Among these 9 articles, 7 articles were published in English and 2 articles in Chinese. The study selection process is shown in Figure 1.
Characteristics of included studies
The detailed characteristics of the included studies, including first author’s name, year of publication, nation, recruitment time, age range of patients, sex (male/female), sample size (CVA/SC), follow-up period, and other parameters, are presented in Table I. All these studies were published in the period from 2000 to 2018. The sample size ranged from 53 to 600. In total, 1223 patients with CVA were included in these studies, and 1437 were patients with SC.
Table I
Characteristics of studies included in the meta-analysis
| Study | Year | Language | Country | Number of patients (female/male) | Age range (mean) | Groups | n | Years of onset |
|---|---|---|---|---|---|---|---|---|
| Li [12] | 2017 | Chinese | China | 86/110 | 6.1 ±1.3 | CVA | 106 | October 2009 to March 2012 |
| SC | 90 | |||||||
| Marchand [13] | 2003 | English | France | 34/19 | 6.8 ±2.3 | CVA | 26 | April 1995 to June 2002 |
| SC | 27 | |||||||
| Juhn [14] | 2008 | English | Korea | 258/264 | 5.7 ±2.4 | CVA | 174 | June 2001 to March 2006 |
| SC | 348 | |||||||
| Jung [15] | 2010 | English | Korea | 258/260 | 6.5 ±3.1 | CVA | 170 | May 2003 to June 2008 |
| SC | 348 | |||||||
| Chan [16] | 2015 | English | America | 312/288 | 5.9 ±1.9 | CVA | 242 | June 2003 to March 2011 |
| SC | 163 | |||||||
| Nantanda [17] | 2013 | English | Denmark | 200/166 | 5.5 ±2.7 | CVA | 203 | August 2011 to June 2012 |
| SC | 163 | |||||||
| Romero-Espinoza [18] | 2018 | English | Germany | 55/65 | 5.2 ±2.9 | CVA | 42 | January 2013 to January 2015 |
| SC | 78 | |||||||
| Nantanda [19] | 2014 | English | Uganda | 180/186 | 5.6 ±2.7 | CVA | 200 | August 2011 to June 2012 |
| SC | 160 | |||||||
| Gui [20] | 2017 | Chinese | China | 54/66 | 6.9 ±2.3 | CVA | 60 | January 2014 to March 2016 |
| SC | 60 |
Quality assessment
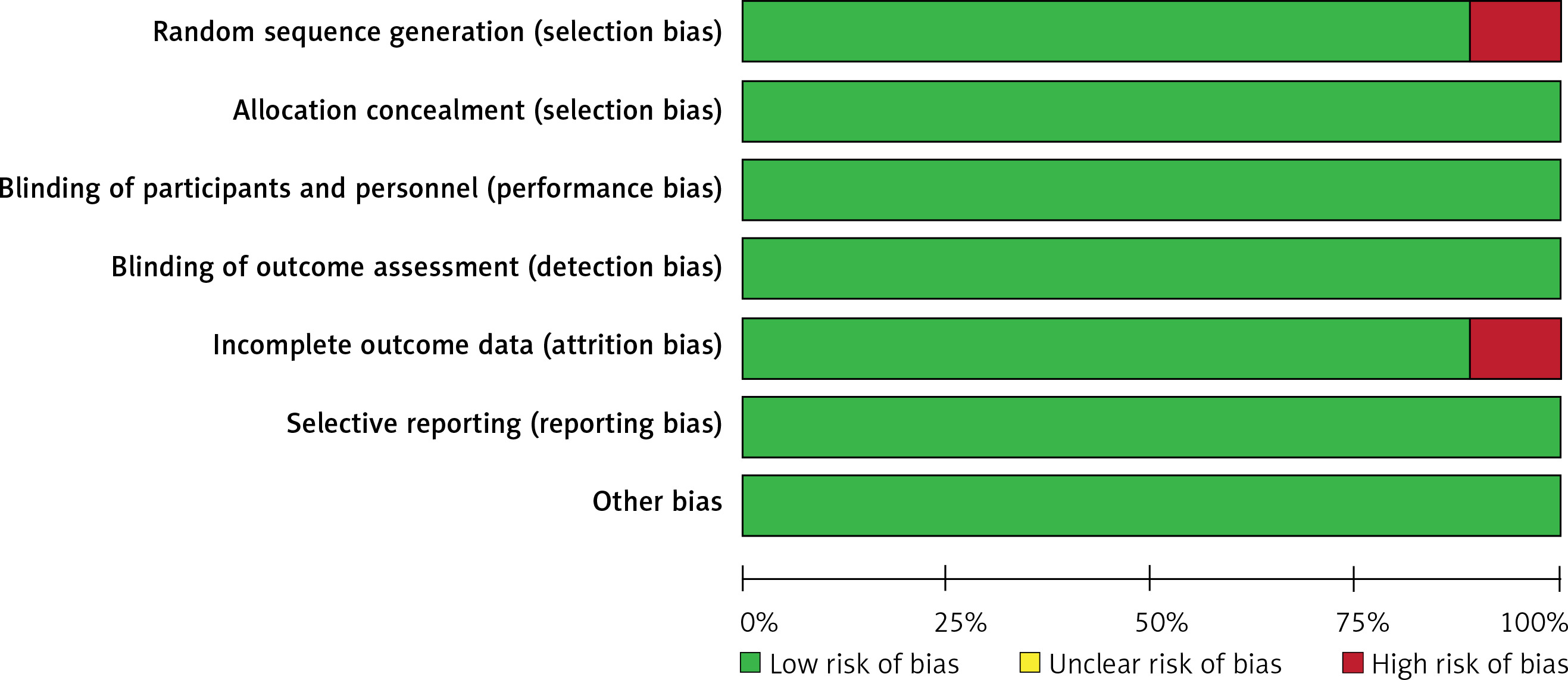
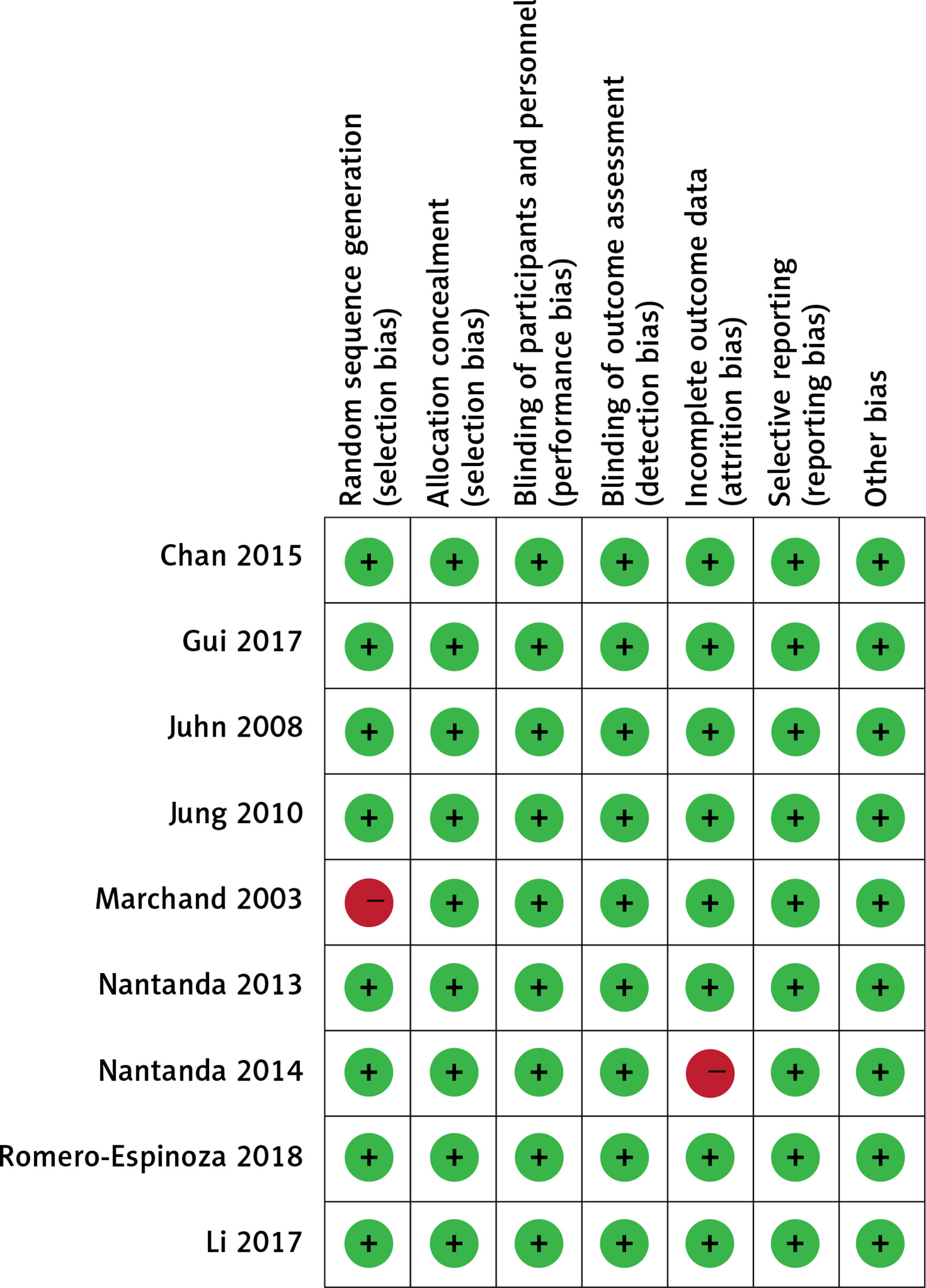
The bias table in the Review Manager 5.2 Tutorial was used to evaluate the risk of each study by applying the criteria for evaluating design-related bias. The evaluation in this study is shown in Figures 2 and 3. In the 9 articles, 1 trial showed a problem in patient selection and 1 showed a problem in attrition bias. Overall, all the trials were free of risk.
Results of meta-analysis
Meta-analysis of serum IgE level in CVA and SC patients
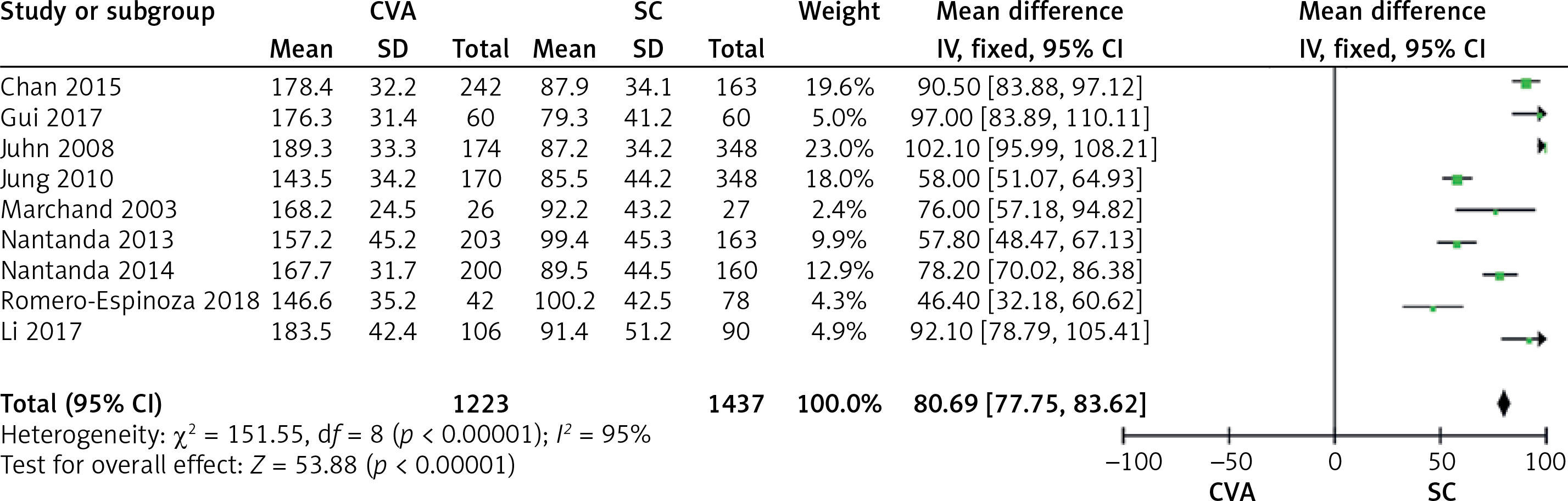
Nine studies compared serum IgE level in CVA and SC patients. The forest plot for serum IgE level in different groups is shown in Figure 4. Total IgE was detected by immunoturbidimetry. All these studies reported that serum IgE levels were statistically significantly different between CVA and SC patients. The value of IgE in CVA patients (MD = 167.85) was higher than that in SC patients (MD = 90.29). The overall result is shown in Figure 4 (MD = 80.69, 95% CI: 77.75–83.62, p < 0.001; p for heterogeneity < 0.001, I2 = 95%).
Meta-analysis of eosinophil count in CVA and SC patients
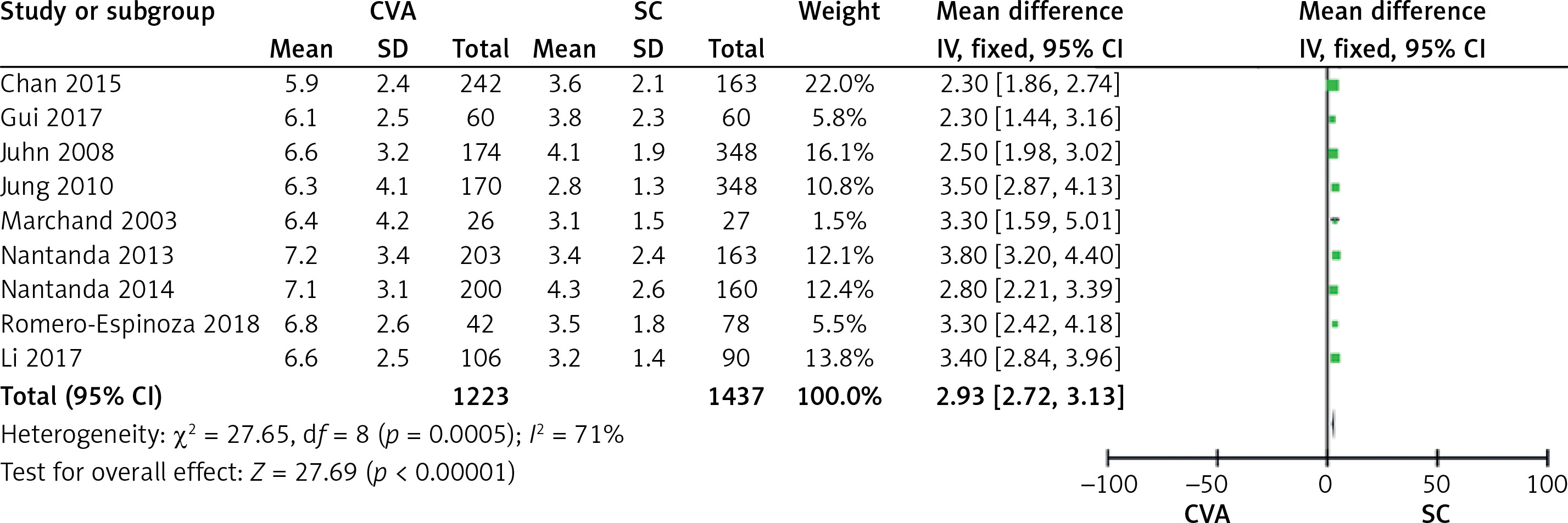
Nine studies comparing eosinophil count showed a statistically significant difference (Figure 5). Eosinophil count was detected by a blood cell counter. The meta-analysis indicated that eosinophil count in patients with CVA (MD = 6.56) was higher than in patients with SC (MD = 3.53) (MD = 2.93, 95% CI: 2.72–3.13, p < 0.00001; p for heterogeneity < 0.001, I2 = 71%).
Meta-analysis of the number of IgM positive CVA and SC patients
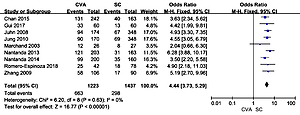
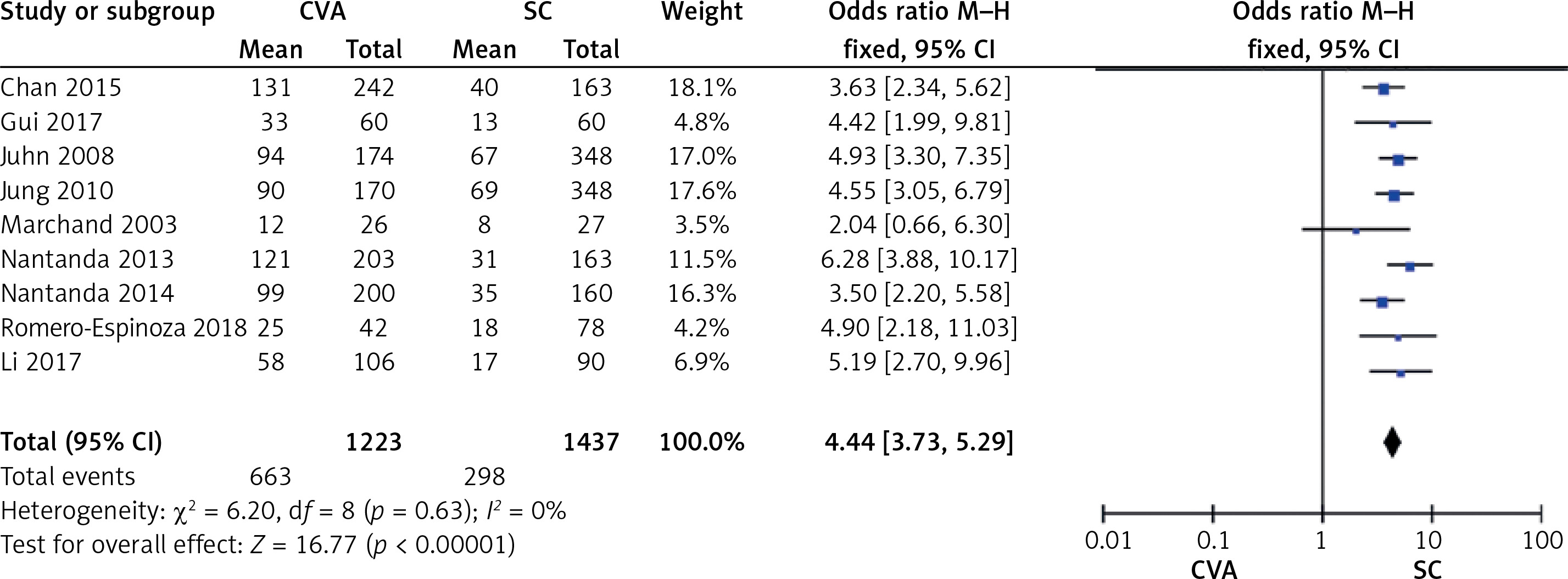
Nine studies compared the number of IgM (anti-IgM for mycoplasma pneumonia) positive CVA and SC patients. The determination of serum IgM was as follows: 2 ml of blood was extracted from children and centrifuged at 2000 rpm. Serum IgM was extracted by passive agglutination, and then frozen in the refrigerator at 15°C and IgM > 1 : 80 was considered positive [7].
The meta-analysis showed a statistically significant difference in the number of positive IgM cases between CVA and SC patients (OR = 4.44, 95% CI: 3.73, 5.29, p < 0.001; p for heterogeneity = 0.63, I2 = 0%) (Figure 6). The number of IgM positive patients in the CVA group (MD = 73.67) was higher than that in the SC group (MD = 33.12).
Sensitivity analysis
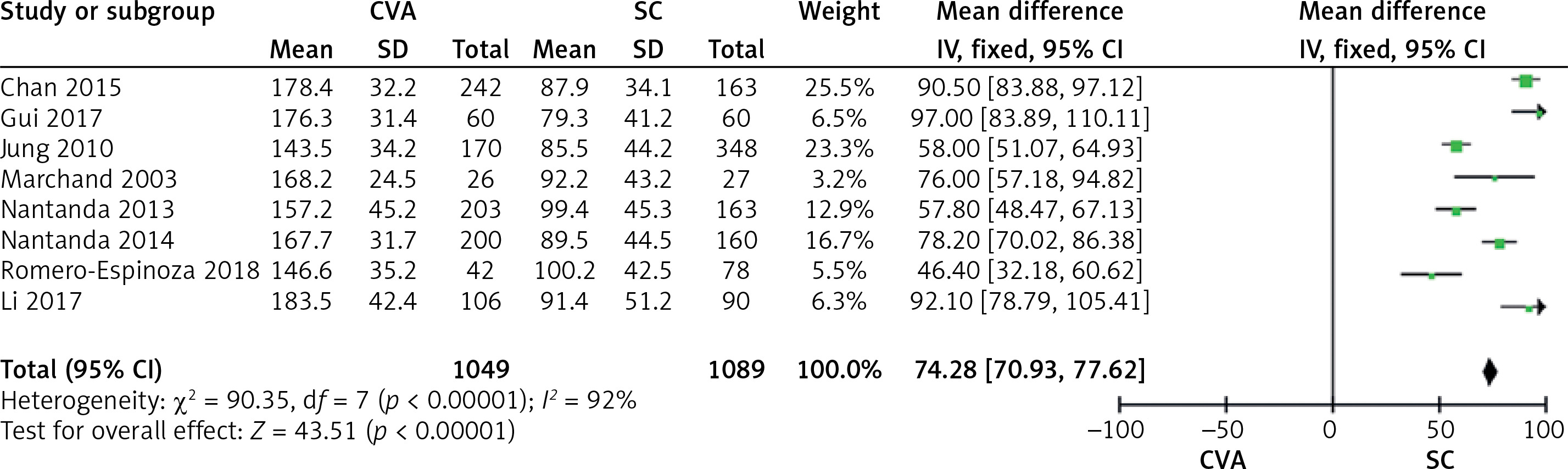
According to the results of the meta-analyses, the heterogeneity of serum IgE level was very high (I2 ≥ 95%). As shown in Figure 7, the high heterogeneity of serum IgE level was probably due to differences in the studies. When the study in 2008 by Juhn [14] was excluded, I2 changed from 95% to 92%, which suggested that the sensitivity of the article was stable.
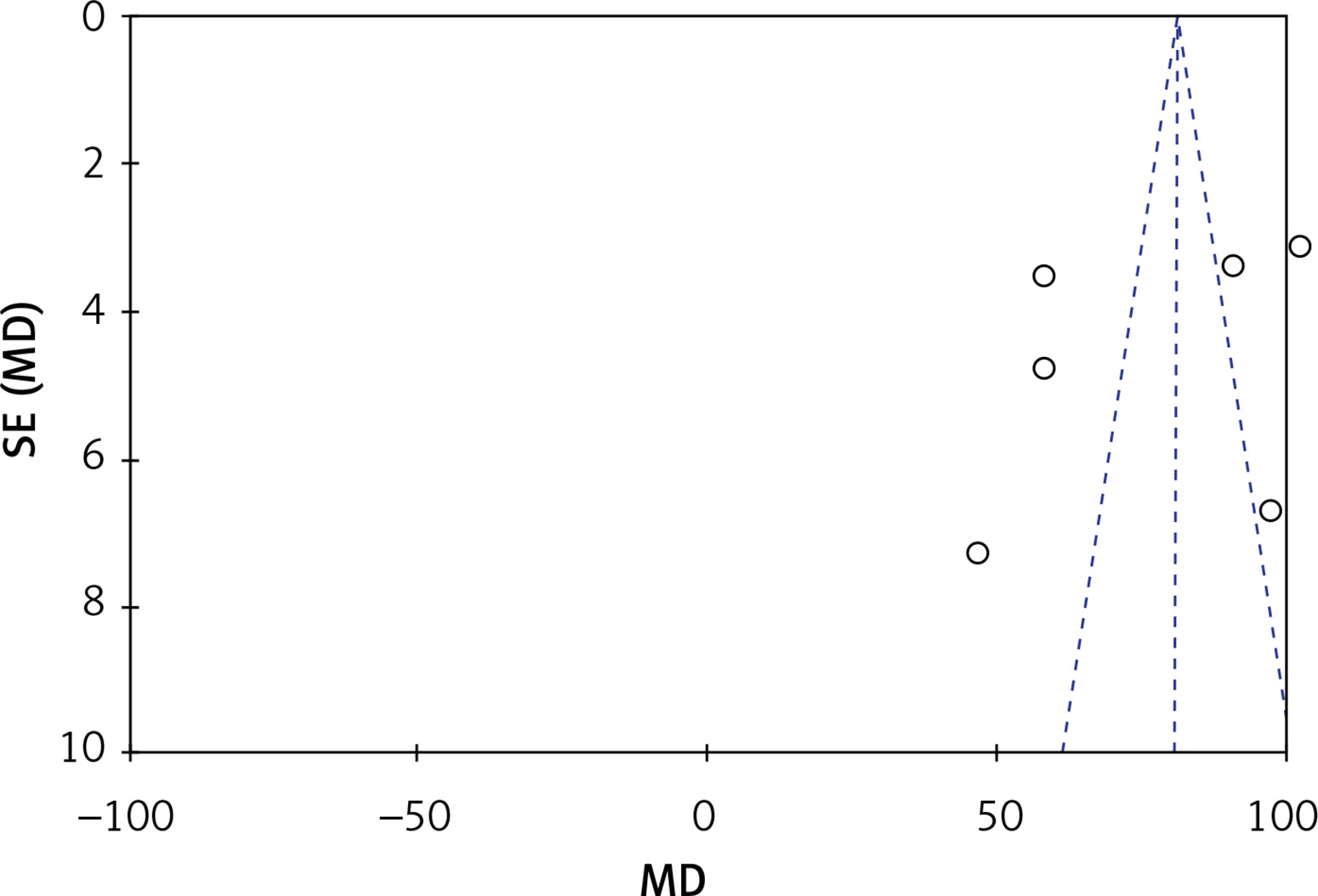
Bias analysis
A funnel plot for serum IgE level in CVA and SC patients was performed. All the studies were included in the plot. The results showed some publication bias since the symmetrical characteristic of the funnel plot was not good (Figure 8).
Discussion
Asthma affects almost 30 million Americans and 300 million persons worldwide. The prevalence of asthma has increased over the past 2 decades in both children and adults [21–23]. CVA is a common cause of emergency hospital visits in low and medium income countries [24, 25]. Outcomes of children with CVA are influenced by age of the child, peripheral oxygen saturation on admission and adherence to asthma therapy.
Pneumonia and CVA are different disease entities with similar clinical presentations among young children. The diagnostic gold standards for pneumonia and CVA in young children are quite sensitive [26, 27]. Pneumonia is considered the major cause of morbidity and mortality among children. Diagnosis is usually based on the presence of cough and/or difficulty in breathing, and rapid breathing with/without chest indrawing.
In the comparison of CVA and SC, IgE level in the CVA group was higher than that of the SC group. Since infection with Mycoplasma pneumoniae was highly related to IgE level, it could be interpreted that CVA was associated with mycoplasma pneumonia. Koh et al. [28] reported that CVA can be secondary to mycoplasma pneumonia, which indicated that CVA and mycoplasma pneumonia had a strong relationship. When patients develop CVA, the possibility of mycoplasma pneumonia should be considered. Laboratory examinations should be carried out as soon as possible, and Mycoplasma pneumoniae should be removed in time.
The eosinophil count in the CVA group was more than that in the SC group, which is also an indicator of mycoplasma pneumonia. This supports the association between CVA and mycoplasma pneumonia.
The number of IgM positive patients was higher in the CVA group than that in the SC group. Mycoplasma pneumoniae would lead to a rise in the number of IgM positive patients. The number of IgM positive patients was not statistically significantly different between the CVA group and the SC group. Therefore, the association between CVA and mycoplasma pneumonia had further confirmation. Gui et al. [29] reported that IgM can be used as a test for children with CVA. For screening CVA in children, eosinophil count and IgE level have high predictive value. Therefore, eosinophil count, IgE and IgM can be combined for early diagnosis of CVA. These articles further support the conclusion of this study.
This study had some limitations. First, more indicators such as gender and stratification of age in both the CVA and SC group should be analyzed since gender and age might influence the results, and will be evaluated in the future. Second, more indicators should be included to comprehensively analyze the results, which could be conducted in future studies. Third, articles from more countries could be included in future studies to guarantee the universality of the association. Fourth, all reported studies used serology to identify Mycoplasma pneumoniae infection, and none used culture or PCR; more identification methods could be included in the future.
In conclusion, based on the results of blood test including IgE, eosinophil count and positive IgM between the CVA group and the SC group, there may be a correlation between CVA and mycoplasma pneumonia, although the causation of mycoplasma pneumonia needs to be further studied. Therefore, comprehensive preventive measures such as avoiding smoke and air pollution should be adopted for CVA among children.